The presence of a certain family of bacteria in the gut microbiota may be involved in the recurrence of Crohn’s disease following bowel resection. Can the presence of these bacteria predict recurrence?
Up to 70% of patients with Crohn’s disease undergo a bowel resection, two-thirds of whom experience a relapse requiring a further operation. The role of the microbiota associated with the intestinal mucosa in the recurrence of Crohn’s disease is well known, but there are currently few data on the luminal environment following bowel resection. A research team carried out a large randomized longitudinal prospective study on 130 patients with Crohn’s disease following surgery with the purpose to investigate the link between the intestinal microbiota and the risk of recurrence.
Enterobacteriaceae and risk of recurrence
An endoscopy was performed 6 months after surgery in two-thirds of the patients, and a colonoscopy at 18 months in all patients, in order to detect recurrence of the disease. Stool samples were taken two weeks before surgery and 6, 12 and 18 months after surgery in order to analyze the intestinal microbiota via sequencing of the 16S rRNA gene. According to the results, abundance of Enterobacteriaceae prior to surgery and 6 months after surgery is associated with an increased risk of recurrence of the disease at 18 months, whereas an increase in bacteria belonging to the Lachnospiraceae family is associated to a reduced risk. The results also showed that while the relative abundance of these bacteria families is important, increased species diversity within a family also contributes to the risk of recurrence.
An environment conducive to relapse
Following surgery, the intestinal environment is altered (exposure to oxygen, change in pH, antibiotics, etc.), leading to a decrease in Lachnospiraceae (obligate anaerobes), some species of which produce butyrate. This decrease is thought to modify the availability and metabolism of butyrate within the colonocytes, leading to a metabolic switch and an increase in oxygen, which, according to the researchers, is responsible for the proliferation of Enterobacteriaceae (facultative anaerobes). Integrating these new data with (sidenote:
De Cruz P, Kamm MA, Hamilton AL, et al. Crohn’s disease management after intestinal resection: a randomised trial. The Lancet. 2015;385(9976):1406–1417
) should provide a full understanding of the disease.
One of the main target organs for SARS-CoV-2 other than the lungs is the intestines, which also act as a potential dissemination route. Hence this review focusing on gastrointestinal disorders and the role of the gut microbiota in Covid-19 symptoms and mortality.
Although Covid-19 primarily affects the lungs, physicians and researchers have quickly focused on the role of the gut microbiota in the disease, particularly since intestinal symptoms (vomiting, nausea, diarrhea) appear to be more common in severe cases, with three meta-analyses involving around 4,000-10,000 patients reporting a prevalence of 10% to 17.6%. The infection triggers an inflammatory bowel reaction, evidenced by high fecal levels of a specific biomarker, calprotectin.
The virus is present in the digestive system
SARS-CoV-2 infects cells mainly by binding to the (sidenote:
Angiotensin-converting enzyme 2
) receptor, which is involved in the homeostasis of the renin-angiotensin-aldosterone system, crucial to the pathophysiology of all organs. ACE2 is strongly expressed in lung tissue, hence the vulnerability of this organ, but it is also expressed in the heart, liver, and intestines. The digestive system may therefore be a gateway for the virus via contaminated food. Fecal-oral transmission may follow. Actually, viral RNA is present in the stool of half of Covid-19 patients, even when the virus is absent from the respiratory tract. In addition, the virus appears capable of replicating in the gut.
Potential mechanisms
Several mechanisms may be involved in the gastrointestinal disorders observed:
• Weakening of the intestinal barrier due to local inflammation or virus replication.
• Deregulation of ACE2, whose deficiency increases gut’s susceptibility to inflammation. SARS-CoV-2 reduces the expression of ACE2 in the lungs and is likely to do so in the gut also.
• Alteration in the composition and functions of the microbiota as a result of hypoxia caused by Covid-19.
• Involvement of gut-brain axis. The enteric nervous system may be affected either via direct viral infection or through an (sidenote:
For example, inflammatory cytokines
), intensifying diarrhea and potentially stimulating the vagus nerve to provoke vomiting.
Dysbiosis of the gut microbiota
An ACE2 deficiency has been shown to alter the composition of the intestinal microbiota in mice, and Covid-19 patients develop an intestinal dysbiosis, with a loss of bacterial diversity and abundance. This dysbiosis has significant consequences: the gut microbiota can remotely stimulate the host’s response to respiratory viral infections; conversely, the dysbiosis can worsen the outcome of the disease, with reduced presence of commensal bacteria favoring the over-representation of pathogenic bacteria. Therefore, the role of the gut microbiota in Covid-19 infections remains to be determined, with the microbiota potentially constituting a biomarker of disease severity or offering therapeutic strategies.
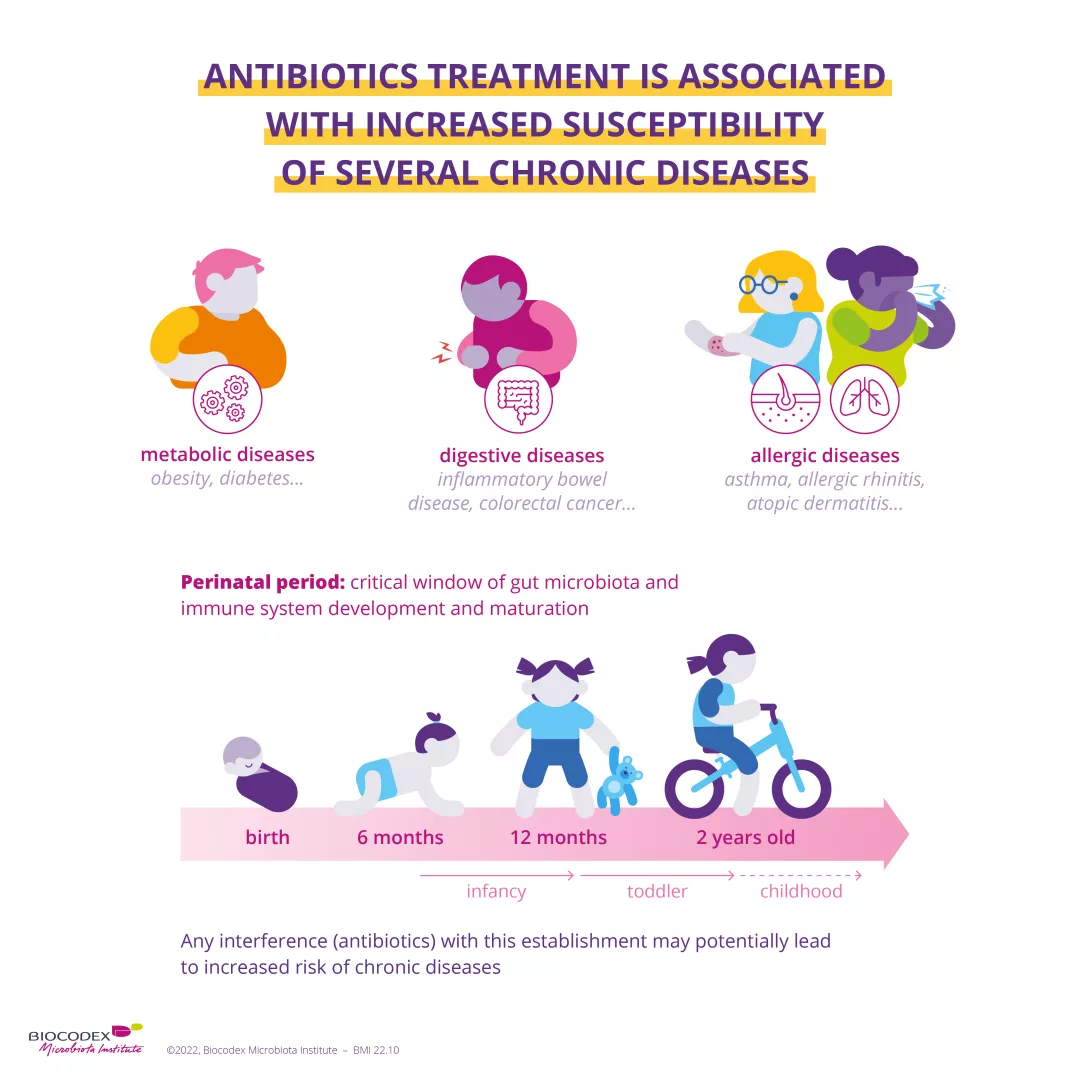
We know that infants exposed to antibiotics are more likely to develop asthma at a later stage in life but science still struggles to explain the mechanisms behind this correlation. One clue seems to be right under our nose, or rather inside it! The nasal microbiota appears to play a central role.
We are often told not to abuse antibiotics, but the use of antibiotics to treat conditions other than bacterial infections is still too common, with consequences for our health. Indeed, exposure to antibiotics during the first months of life may be associated with the subsequent development of asthma, an inflammatory disease of the (sidenote: https://www.who.int/news-room/q-a-detail/asthma). Alterations in the intestinal and nasal microbiota are recognized as a risk factor for the development of the disease and an indicator of its severity. Knowing that antibiotics alter bacterial communities, a team of researchers considered whether alterations of the nasal microbiota can explain the development of childhood asthma.
Image
Antibiotics save life! Did you know that they also have an impact on your microbiota? Did you know that the misuse and overuse of antibiotics can lead to antibiotic resistance? Have you heard about the World AMR Awareness Week (WAAW)? All the answers in this dedicated page:
A team studied a group of around 700 children to search for a link between antibiotic exposure before the age of one and the development of asthma at the age of seven. In total, half of the children had received antibiotics in their first eleven months and almost 8% of them subsequently developed asthma. This proportion rose to over 11% among those treated with two or more antibiotics before eleven months, an increase of 4% compared to the children not exposed to antibiotics.
The researchers observed that the nasal microbiota changes during the first two years of life and that antibiotic therapy before the age of one impacts babies’ nasal flora, with this impact growing as the number of treatments increases. In particular, the absence from the nose of Moraxella–a bacterium often associated with respiratory diseases–seemed to signal an early and significant exposure to antibiotics. Their use before the age of one may therefore have long-term harmful effects on the nasal microbiota, facilitating the cascade of events that lead to the development of asthma. Even if other factors, such as the intestinal microbiota or the immune system, are also involved, these results still support current recommendations for the prudent use of antibiotics, especially among infants.
What is the World AMR Awareness Week?
Each year, since 2015, the WHO organizes the World AMR Awareness Week (WAAW), which aims to increase awareness of global antimicrobial resistance.
Antimicrobial resistance occurs when bacteria, viruses, parasites and fungi change over time and no longer respond to medicines. As a result of drug resistance, antibiotics and other antimicrobial medicines become ineffective and infections become increasingly difficult or impossible to treat, increasing the risk of disease spread, severe illness and death.
Held on 18-24 November, this campaign encourages the general public, healthcare professionals and decision-makers to use antibiotics, antivirals, antifungals and antiparasitics carefully, to prevent the further emergence of antimicrobial resistance.
By short-circuiting the stomach or removing part of it, bariatric surgery significantly alters the gut microbiota. However, results seem to depend on the technique used.
Global prevalence of obesity almost tripled between 1975 and 2016 and now represents a major public health issue. Bariatric surgery is currently the best strategy for achieving lasting weight loss in patients suffering from morbid obesity1, with a five-year success rate of over 66%. It mainly consists of two techniques of comparable effectiveness: gastric bypass (or more precisely, laparoscopic Roux-en-Y gastric bypass) and sleeve gastrectomy, which involves removing two-thirds of the stomach. How do these interventions affect the bacterial ecosystem? Do the two approaches have the same impact?
Enriched and diversified intestinal microbiota
To find out, researchers compared two groups of around 100 patients, one subjected to gastric bypass and the other to sleeve gastrectomy. Six months later they observed a significant increase in bacterial abundance and diversity in the gut microbiota of all participants. 40% of bacteria were common to both approaches, including Akkermansia muciniphila–known to be negatively correlated with obesity–, as well as certain proteobacteria such as Escherichia coli, suspected of influencing both appetite and metabolism after surgery. However, only the gastric bypass caused a depletion of Faecalibacterium prausnitzii, a species associated with certain metabolic disorders and inflammatory bowel diseases.
Gastric bypass has a greatest impact
Both approaches also resulted in increased transport systems for vitamins B12 and B1, manganese, iron, and zinc, suggesting increased use of these nutrients by bacteria. According to the authors, the impact of gastric bypass was greater than that of sleeve gastrectomy in all aspects. However, they consider that a further three to five years will be required to establish whether these discoveries have the clinical ability to preferentially direct patients towards one treatment or the other.
1. Morbid obesity is defined by a body mass index (BMI) of over 40
Farin W, Oñate FP, Plassais J, et al. Impact of laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy on gut microbiota: a metagenomic comparative analysis [published online ahead of print, 2020 Mar 20]. Surg Obes Relat Dis. 2020;S1550-7289(20)30132-5. doi:10.1016/j.soard.2020.03.014
Inflammatory bowel diseases (IBDs) include Crohn’s disease and ulcerative colitis. These diseases don’t have an effect on life expectancy, but they do significantly alter quality of life. Treatment plans are starting to target microbiota.
IBDs, Crohn’s disease and ulcerative colitis (UC), are characterized by inflammation in the wall of part of the digestive tract, which is related to hyperactivity of the digestive immune system. During IBD flares, the most common symptoms are abdominal pain and diarrhea, which can sometimes be hemorrhagic. These diseases can also present signs in systems outside the digestive tract, including joints and the ophthalmic, cutaneous, and hepatic systems.
IBDs affect 1 person in every 1000 in Western Europe and most often appear between 20 and 40 years of age. These illnesses follow intermittent courses, with alternating periods of flares and remission. In Crohn’s disease, this inflammation can be localized at all stages of the digestive system, from the mouth to the anus, although it is most often found in the intestine. Ulcerative colitis is localized in the rectum and colon.
Multifactorial disorders
The causes of IBDs include genetic predisposition, environmental factors like pollution and diet, the immune system, and intestinal microbiota. IBDs may also be caused by a lack of exposure to microorganisms during childhood due to an excessive hygiene, for example.
Modified intestinal content
Intestinal microbiota seems to play an important yet still poorly understood role in the characteristic inflammation of IBDs. Numerous studies have observed dysbiosis in these patients, i.e. a change in the microbiota equilibrium, linked to genetic and environmental factors. Anti-inflammatory bacteria in particular are weakened. This imbalance changes the content of the intestine and can lead to chronic inflammation.
Hope for treatment
There is no curative therapy, but anti-inflammatories can limit painful flares. Treatment currently includes corticosteroid therapy, treatments called “immunomodulators” that can reduce the immune system’s reactions, like anti-TNFα, and surgery in 80% of Crohn’s cases and 20% of UC. It rarely provides a definitive cure. Researchers are currently trying to target the role of microbiota in IBDs, trying to reduce the presence of pathogens and boost the growth of good microorganisms.
Allergic eczema, or atopic dermatitis, is a skin disease combining cutaneous dryness and itching. Not contagious, this cutaneous condition is made more likely by a predisposition to allergies, in which microbiota plays an important role.
Three times more common than 30 years ago, today, eczema affects up to 20% of children. It has become the most common childhood cutaneous condition in industrialized countries. However, in the majority of cases, eczema disappears in adolescence, and only 10 to 15% of patients remain affected throughout their lives.
An excessive immune response
Eczema is related to a genetic predisposition that alters the skin barrier. This alteration paves the way for allergens to penetrate into the skin, which causes an excessive immune reaction. Changes in the composition and diversity of the intestinal and cutaneous microbiotas observed in these patients may also be involved.
Eczema manifests very early in infancy (between 1 and 3 months) by rough, dry skin, and the appearance of very itchy red patches during inflammatory flares.
Limit skin irritation
Treatment for eczema primarily tries to limit skin irritation (wearing cotton clothes, using gels without soap, being gentle when washing your skin, etc.) and to reduce cutaneous lesions with hydrating creams and topical steroids. In the most severe cases, the doctor may prescribe short-term antihistamines.
Probiotics improve symptoms
Another approach: correct the dysbiosis (imbalance in bacterial flora) by modifying the intestinal and cutaneous microbiotas. Several studies have shown that probiotics improve eczema symptoms (particularly certain lactobacilli) and reduce intestinal inflammation in affected babies. Given as a preventative treatment to pregnant women, they could reduce the frequency of symptoms in their baby.
Asthma is a common chronic respiratory disease that affects both adults and children. Over 260 million people suffer from the disease worldwide1 and it is the most common chronic disease in children.1 Uncontrolled asthma, the most debilitating form of the disease, has serious consequences for patients’ day-to-day lives. The discovery that the gut, lung and nasal microbiota are involved in the development of asthma opens up new therapeutic avenues. Explanations below.
Asthma is a chronic disease of the respiratory system that manifests itself as coughing, wheezing, shortness of breath, tightness in the chest, or a combination of these symptoms.1 Symptoms are caused by a narrowing of the airways in the lungs due to inflammation of the bronchi.1 Asthma attacks occur more frequently at night or during physical activity and the severity and frequency of attacks vary from patient to patient.1
Did you know that…
Asthma affects children more than adults. However, death from the disease is more common in adults.2
Childhood asthma is more common in boys, but in adulthood the disease is more common in women.2
Predispositions and triggers for asthma
Asthma is a complex multifactorial disease. It can develop due to a genetic predisposition (allergic background) and/or exposure to environmental factors such as allergens (pollens, mites), tobacco smoke or air pollution. Strong emotions, cold air or physical exercise can also trigger attacks. Lastly, individual-specific factors, such as an infection, or even obesity, can also come into play.2
Link with the microbiota?
Numerous studies note the role played by the various microbiota in the disease:
Gut microbiota
Reduced gut microbiota diversity, i.e. an imbalance in gut microbiota composition (known as (sidenote:
Dysbiosis
Generally defined as an alteration in the composition and function of the microbiota caused by a combination of environmental and individual-specific factors.
Levy M, Kolodziejczyk AA, Thaiss CA, et al. Dysbiosis and the immune system. Nat Rev Immunol. 2017;17(4):219-232.)), in the first years of life is associated with an increased risk of developing asthma later in childhood.3 Some researchers believe that analyzing an infant’s gut microbiota could predict the risk of developing the disease.4 One factor behind such imbalances that has received much attention is the impact of antibiotics taken in the first weeks or months of life, i.e. when the gut microbiota and immunity are developing.5 Some studies have shown a link between antibiotic use and an increased risk of asthma later in childhood.6 Moreover, one research team has recently suggested that a gut dysbiosis in infants exposed to antibiotics may be responsible for childhood asthma.7 However, this mechanism has yet to be confirmed.
Lung microbiota
The lung microbiota is also thought to play a role, and although our understanding in this area is still very limited, it is a rapidly expanding field of research.8 The discovery of a unique lung flora with signatures specific to patients suggests a role in asthma.9,10 Furthermore, it appears that respiratory function in moderate to severe asthma is associated with the degree of lung inflammation and the composition of the microbiota.11,12 While research to confirm these results is ongoing, characterizing the bacterial populations living in the lower respiratory tract may help improve patient management or even better predict attacks.10
Nasal microbiota
Data relating to the nasal microbiota are also very limited. However, an imbalance in the composition of the nasal microbiota has also been associated with the disease,13 and even with the severity of attacks,14 although no causal relationship has been established. Lastly, as with the gut microbiota, a very recent study on 700 children suggests that an alteration of the nasal microbiota due to antibiotic treatment before the age of 1 could explain the onset of childhood asthma at 7 years of age.15 However, this remains to be confirmed.
Living with asthma: treatments and solutions?
Although asthma cannot be cured, there are treatments that allow asthma patients to lead normal and active lives. Symptomatic treatments mainly limit the intensity of acute attacks by opening the bronchi, while disease-modifying treatments reduce inflammation of the airways, thus improving respiratory function and reducing attack severity.1
Studies on the relationship between the microbiota and asthma suggest that modifying the microbiota could help prevent the disease, leading researchers to focus their efforts on the use of probiotics and prebiotics.16,17 Their use as a treatment for the disease is also being studied.18
Are there any protective factors?
Exposure to (sidenote:
Microorganisms
Living organisms that are too small to be seen with the naked eye. They include bacteria, viruses, fungi, archaea and protozoa, and are commonly referred to as “microbes”.
What is microbiology? Microbiology Society.) during early childhood seems to help prevent asthma. Contrary to popular belief, living in a sanitized environment does not necessarily protect against respiratory diseases. Some studies show that house dust is not necessarily a risk factor for the development of the disease,19 while others have shown a decreased risk of asthma in children born and raised in the countryside20 or with pets.21
This article is based on scientifically approved sources. However, if you or your child display symptoms, please consult your family doctor or pediatrician.
Allergic rhinitis, or hay fever, is the most common manifestation of respiratory allergy. It is caused by an abnormal and excessive immune response when the organism encounters a foreign substance or a substance to which it has become sensitive. Allergic rhinitis is associated with dysbiosis of the ENT microbiota and gut microbiota.
Tickling sensations, sneezing fits, watery eyes, itching, a blocked or runny nose... Although very common, allergic rhinitis has a real impact on sufferers’ quality of life. Approximately 400 million people suffer with this respiratory allergy1.
Allergic rhinitis is described as seasonal (known as “hay fever”) when it is linked to tree, grass, or herbaceous pollens. It is described as perennial when it is due to allergens that are present all year round, such as dust mites, molds, or animal hair (cats and dogs) 2.
40%
Allergic rhinitis is thought to affect up to 40% of the global population with a high prevalence.
The symptoms of allergic rhinitis
Allergic rhinitis has very characteristic symptoms, usually a combination of 3:
Pruritus (itching, irritation)
Anosmia (loss of smell)
Rhinorrhea (runny nose)
Repeated sneezing
Nasal obstruction (blocked nose)
In seasonal allergic rhinitis and perennial allergic rhinitis, these symptoms are exacerbated.
Modified microbiota
Imbalances in the gut microbiota and in the ENT microbiota (ear-nose-throat microbiota), also known as “dysbiosis”, have been demonstrated in cases of allergic rhinitis. This dysbiosis is characterized by a low diversity of the gut microbiota4,5, and a composition of the ENT microbiota (ear-nose-throat microbiota) that differs from that of healthy individuals 6-8. Finally, all the factors that can impact the gut microbiota (antibiotics, diet, etc.) during the perinatal period may have long-term effects on allergy susceptibility 9.
Treatments for allergic rhinitis
The treatment of allergic rhinitis is based on 3 approaches: avoidance of allergens, medication and desensitization. There are also symptomatic treatments to improve comfort 10. Finally, the approach of correcting (sidenote:
Dysbiosis
Generally defined as an alteration in the composition and function of the microbiota caused by a combination of environmental and individual-specific factors.
Levy M, Kolodziejczyk AA, Thaiss CA, et al. Dysbiosis and the immune system. Nat Rev Immunol. 2017;17(4):219-232.)and rebalancing the microbiota with probiotics is being studied, with promising results. These probiotics seem to be effective in improving the symptoms of allergic rhinitis and enhancing patients’ quality of life 11.
Food allergies are a constantly progressing phenomenon and remain difficult to treat. However, new therapies are coming to light with the discovery of the involvement of the microbiota.
Food allergies are a dysfunction in the immune system, which reacts abnormally immediately after ingestion of a specific food. The food, normally harmless to the body, is then called an “allergen.” These allergies affect 3% of the general population and 5% of children.
Many foods to blame
Products likely to trigger a food allergy are numerous and vary according to age and the person’s food habits. Governmental sites regularly update the list of identified allergens. Children are more sensitive to eggs, peanuts, and cow’s milk, whereas adults are more sensitive to crustaceans and mollusks, certain fruits, and soy.
In contrast with food intolerances, food allergy symptoms appear violently: they can be digestive, respiratory, or cutaneous. Angioedema, asthma attacks, and anaphylactic shock are life-threatening emergencies.
Imbalance in the microbiota
It has not yet been explained why certain foods cause an inappropriate immune reaction. Studies very quickly established a connection between these allergic phenomena and an alteration in the microbiota: allergic patients all have a different microbiota compared to healthy individuals. Observations of dysbiosis in affected people have shown that certain bacteria are responsible for the appearance of hypersensitivity to dietary proteins.
Probiotics as prevention?
Although the primary treatment for food allergies is removing the offending food, numerous studies have suggested that modulating the microbiota with probiotics and prebiotics may prevent the development of allergies.
Liver diseases (hepatopathies) present varying degrees of severity, ranging at one extreme from steatosis, which is benign and reversible, to hepatic inflammation (NASH), hepatitis, fibrosis, cirrhosis and, at the other extreme, to hepatocellular carcinoma (liver cancer). Asymptomatic in their less serious forms, liver diseases can present with jaundice, nausea, and fever in their advanced forms.
Alcohol abuse is a known cause of diet-based liver disease (alcoholic liver diseases or ALD), however excess weight and obesity are less well-known. The metabolic steatosis (or NAFLD) that they cause represents the primary cause of chronic liver diseases in industrialized countries.
Intestinal dysbiosis, cofactor in liver disease
It seems that these risk factors are not enough to induce hepatopathy on their own. The existence of an imbalance in the intestinal microbiota is also involved. The evidence for this is that all patients with liver disease, regardless of the cause, present with dysbiosis and a change in the intestinal barrier. The more serious the liver damage, the more significant the dysbiosis.
Probiotics, prebiotics, and fecal transplant, three promising avenues for research
Current treatment for liver disease includes lifestyle and diet changes (weight loss and physical activity), with or without associated medical treatments, which can range in complexity (medication, liver transplant).
The role of the microbiota is now clear, so modifying it with prebiotics, probiotics, and fecal transplant constitutes a promising avenue for preventative and therapeutic research.