A risk factor for many diseases... whose causes are not that easy to grasp
"All disease begins in the gut" claimed Hippocrates, the father of modern medicine. And obesity seems to live up to this adage. While it is widely accepted that poor eating habits and a sedentary lifestyle are associated with this epidemic, its potential links to other factors (including gut microbiota) are currently being studied. Obesity has tripled since 19751, with those affected still too often accused of lacking willpower and stigmatized by societal norms. Such simplistic reasoning has probably prevented this global scourge from being taken seriously for a long time despite its serious socio-economic consequences and being the top risk factor, followed by smoking, for premature mortality attributable to an unhealthy lifestyle1.
The gut microbiota
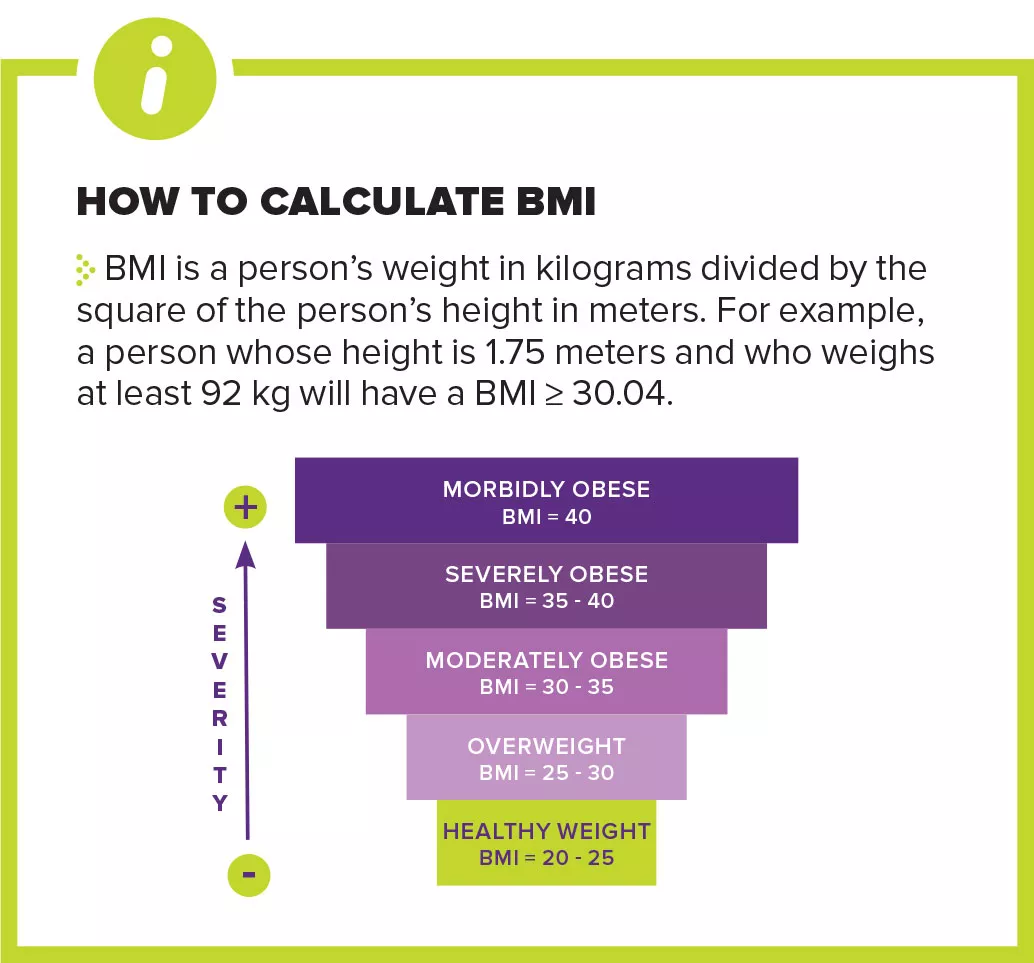
At a time when more people around the world die from over-eating than under-eating, obesity is defined as excessive fat accumulation in the organism1. It is defined by a body mass index (BMI) equal to or greater than 30. Between 1975 and 2014, the prevalence of obesity among adults increased by 7.6% in men and 8.5% in women1. However, such data covers up significant disparities. For example, the prevalence of obesity in Japanese adults is under 4% while the United States has ten times that number. While almost all countries are facing this pandemic (some regions of the world show particularly marked increases2), only Japan, North Korea and some Sub-Saharan countries still have low obesity rates1.
13 % of adults in the world are obese (between 10% and 30% in Europe)
39 % of adults are overweight (between 30% and 70% in Europe)
3,7 % of adults in Japan are obese, against
38,2 % in the United States
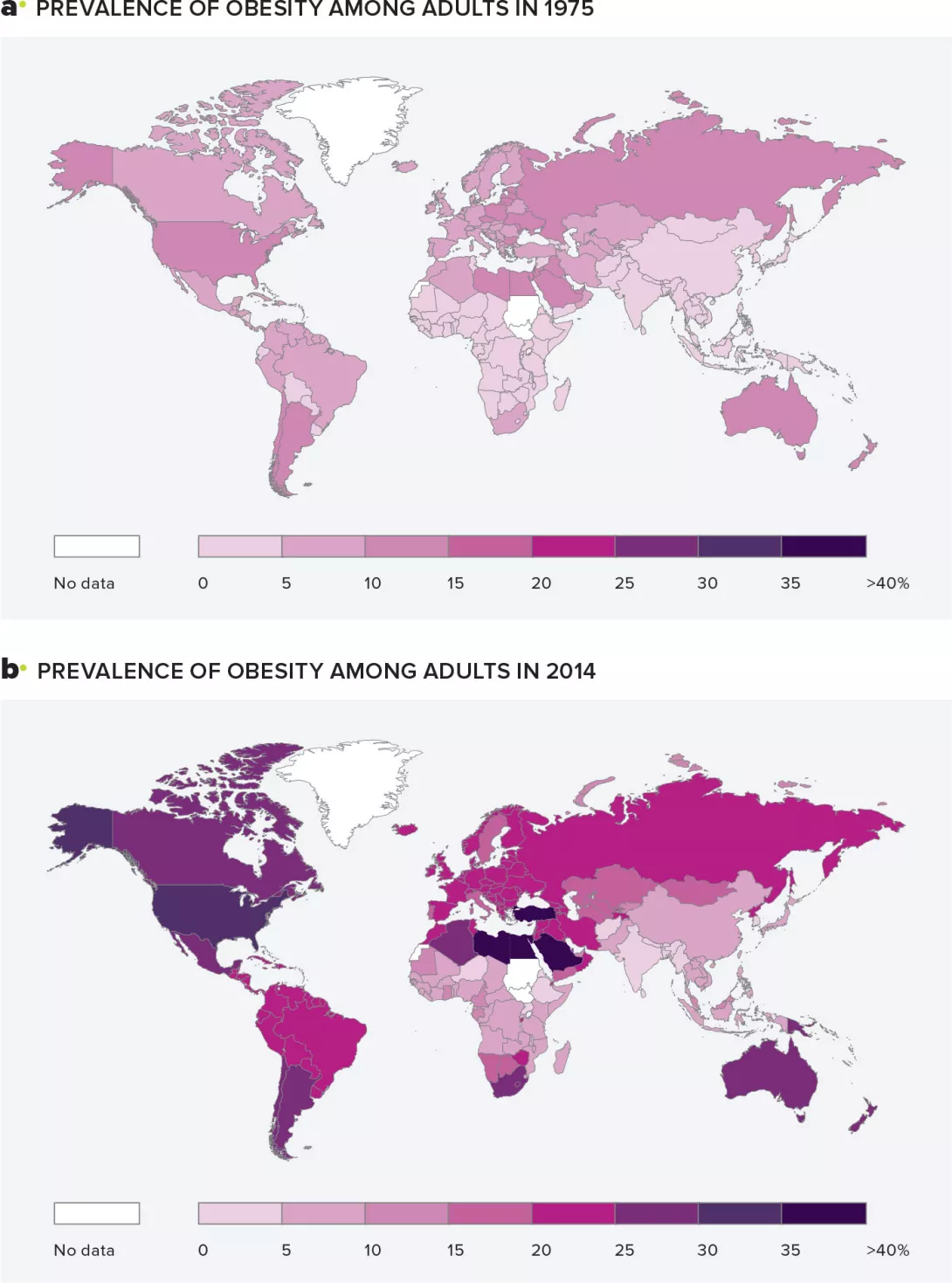
Increase in the number of obese adults over the years. Prevalence of obesity among adults by country in 1975 (a) and 2014 (b). The number of obese adults rose significantly between 1975 and 2014. Global Health Observatory (GHO) database.
A risk factor for many diseases...
The consequences of excess weight are not all apparent at first glance. But the science backs it up—people who are obese have a higher risk of developing other diseases (metabolic disorders like type 2 diabetes, cardiovascular diseases3, depression, some types of cancer, etc.). In addition, men who are overweight have an increased risk of developing urinary disorders and erectile dysfunction, along with a drastically reduced quality of life4. Overall, obese people can expect to live 7 fewer years compared to those of normal weight4.
...whose causes are not that easy to grasp
Absorbing too many calories, particularly fats and sugars, relative to actual energy expenditure is the main and now well-known cause of obesity and excess weight1,5. Yet sometimes adopting healthy behaviors (good nutrition, physical activity, etc.) is not enough to reabsorb the excess weight1. What are the hidden causes?
First off, genetic factors: programmed to withstand hard times (famine for example), human beings inherited genes that enhance their ability to store calories1. Studies on mice and humans even suggest that obesity (including its most severe forms) could be hereditary in 40% to 70% of cases1. However, obesity-associated genes cannot alone explain the current epidemic.
Genes can also be influenced by the environment. As it profoundly affects our behaviors, the environment certainly plays an important role in determining an individual’s build. The increase in the obesity rate over the past 50 years has coincided with changes in our lifestyle, including extremely high levels of fat, sugar and salt in processed foods; increased consumption of fast food and snacks; altered work-life balance; lack of physical activity; lack of sleep or reduced quality of sleep; social stress, etc 1. Daily routines that over time could have caused changes to genes that are passed down and predisposed future generations to an increased risk of obesity: such mysteries are referred to as “epigenetics”1…
The gut, at last. As the body’s true “second brain”, it communicates with our gray matter via an axis that monitors metabolism, i.e. the balance between energy intake and energy expenditure6. When it malfunctions as in obese people, it becomes unable to regulate appetite, satiety and energy storage7,8. Studies confirm that when mice are deprived of gut microbiota and subjected to a high-fat diet, they do not gain weight. In contrast, in animals with intestinal flora, the same diet leads to weight gain7. More surprisingly, if a lean mouse receives a microbiota transplant from an obese subject, it will in turn gain weight. Cause or consequence? For now, researchers are struggling to find answers and identify the underlying mechanisms5,8.
1 Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019
2 Bangladesh, Bhoutan, Inde, Népal et Pakistan, Indonésie, Philippines, Malaisie, Vietnam, Thaïlande, Sri Lanka, Belize, Cuba, République Dominicaine, Porto Rico, Argentine, Brésil, Chili, Paraguay, Uruguay
3 Abenavoli L, et al. Gut Microbiota and Obesity: A Role for Probiotics. Nutrients. 2019 Nov
4 Barathikannan K, et al. Gut Microbiome Modulation Based on Probiotic Application for Anti-Obesity: A Review on Efficacy and Validation. Microorganisms. 2019 Oct
5 Maruvada P, et al. The Human Microbiome and Obesity: Moving beyond Associations. Cell Host Microbe. 2017 Nov
6 Cerdó T, et al. The Role of Probiotics and Prebiotics in the Prevention and Treatment of Obesity. Nutrients. 2019 Mar
7 Lee Clare J, et al. Gut microbiome and its role in obesity and insulin resistance. Ann N Y Acad Sci. 2020
8 Torres-Fuentes C, et al. The microbiota-gut-brain axis in obesity. Lancet Gastroenterol Hepatol. 2017 Oct