Expert Interview : Pr Harry Sokol
Professor Harry Sokol is a hepatogastroenterologist at the Saint- Antoine Hospital (Paris, France). He is also the chairman of the French Group of Fecal Microbiota Transplant (GFTF). Though he understands why this therapeutic approach– still in its infancy–is gaining popularity, he explains the obstacles it is facing.
The gut microbiota Fecal transplant
Fecal microbiota transplant: a miracle cure?
The frenzy surrounding fecal microbiota transplant (FMT) is real and it needs to be slowed down a bit: some patients have unrealistic expectations regarding the benefits of FMT in their particular case. Every week I receive dozens of letters about anything and everything. However, FMT is a not a magical cure! For now, it is indicated to treat a single disease: recurrent C. difficile infection. For all other indications, it is just a potential therapeutic avenue which cannot replace current treatments. Moreover, the future most likely lies in treatments combining stool transplant (or other therapies that target the microbiota) and more standard treatments that target the immune system, for instance.
Why does C. difficile respond that well to fecal microbiota transplant?
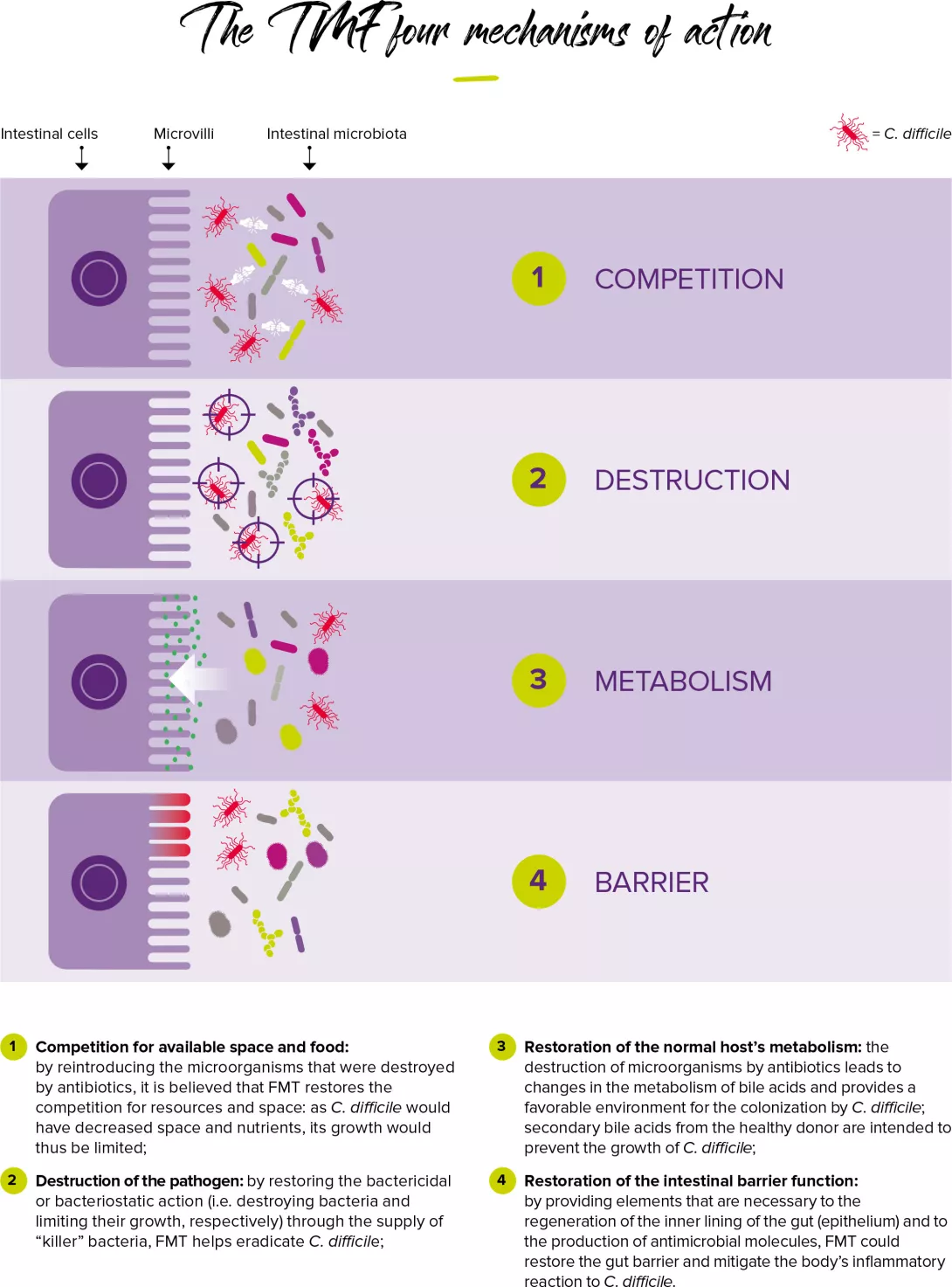
This infection is almost exclusively related to a disruption in the gut microbiota, while in other diseases, the role of the gut microbiota–although presumed– is only one of several contributing factors and its importance probably varies significantly from one disease to another. For instance, in the case of ulcerative colitis, for which we have the strongest data: clinical trials indicate a 20 to 30% rate of remission within a 8-12 week period; which is good, but very far from the results obtained in C. difficile infections (near 90%). This clearly shows that other factors (immune, genetic...) also play a role.
Are there obstacles to the development of clinical research focused on FMT?
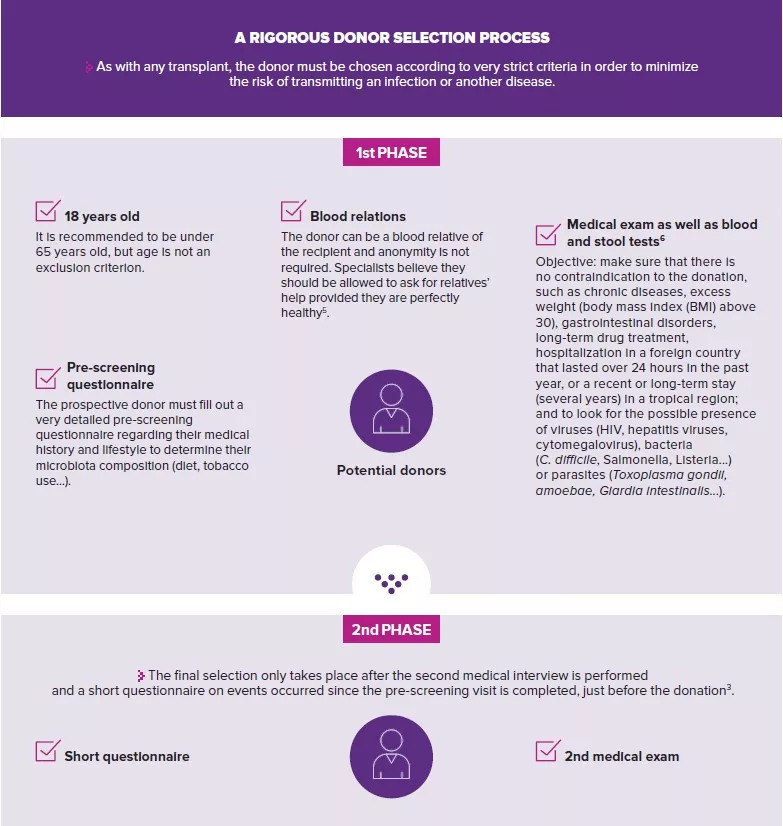
Research on FMT is still at a very early stage since it started less than 10 years ago; which is why we must take the time needed to assess it properly. In France, the handling of feces is subjected to major regulations and the selection of donors is strictly regulated. As a result, clinical trials are expensive and require complex logistics. In addition, since hospitals do not automatically assign a budget to FMT, the mobilization of health professionals varies from one facility to another, thus depriving researchers from a specific structure to rely on. It is time for public authorities to better understand this issue and to invest in order to provide hospitals with the means to develop this line of research. In Assistance Publique-Hôpitaux de Paris (Paris public hospital system), we hope to quickly see the emergence of a structured approach to FMT in the healthcare system.
 Fecal transplant: a promising route?
Fecal transplant: a promising route?
 Improving the definition of stool banks to promote the widespread adoption of FMT
Improving the definition of stool banks to promote the widespread adoption of FMT