The composition of pancreatic tumor microbiome, which is impacted by the gut microbiota, could modulate the patient’s immune response and the growth of adenocarcinoma. Could this discovery rekindle the interest in fecal transplants?
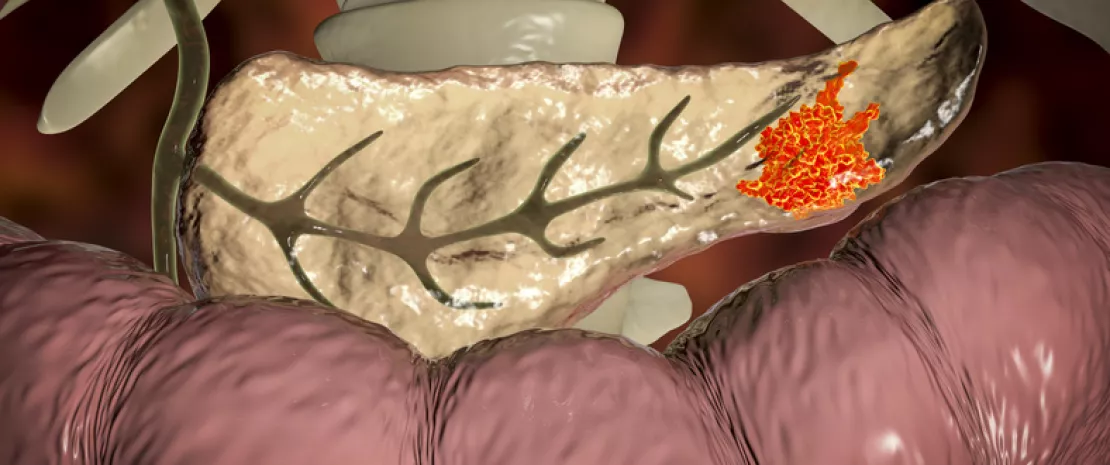
Pancreatic ductal adenocarcinoma (PDAC) is a dreaded cancer. As it is usually detected late, its prognosis is grim, with a 5-year overall survival rate of 9%. The tumor microbiota seems to play a role in this survival rate, based on the numerous results published in Cell by 31 researchers–mainly Americans.
More diversity = longer survival
To understand the impact of tumor microbiota and immune system on the long-term survival rate, these researchers analyzed the composition of the microbiota of resected tumors in 68 patients with PDAC divided into two groups: 36 patients who survived more than 5 years (mean: 10.1 years) and 32 patients who died less than 5 years after the procedure (mean: 1.6 years). Their results put forward a larger diversity of bacterial species present in the tumor microbiota of patients who survived more than 5 years. These results were confirmed by researchers in a second cohort.
Immune modulation
Moreover, the authors highlighted that each one of the two groups of patients displayed a specific intratumoral microbiota signature: presence and abundance of 3 bacterial genera (Pseudoxanthomonas, Streptomyces, Saccharopolyspora) and of Bacillus clausii are able to predict the survival in 97.51 to 99.17% of cases (according to the cohort). Additional immunohistological analyses suggest that the composition of the tumor microbiota could have an impact on cancer development by modulating the anti-tumor immune response through the recruitment and activation of CD8 T cells.
From the intestines to the tumor
In parallel, the analysis of stools, resected tumor tissues and adjacent non-cancerous tissues of three patients showed that the gut microbiota represents about 25% of the tumor microbiota, while it is absent from adjacent tissues: the tumor microbiota could thus be colonized by the gut microbiota. Finally, fecal microbiota transplants (FMT) from three types of patients (long-, short-term survival or control) were carried out in mice. These works confirmed the ability of the gut microbiota to colonize pancreatic tumors. They also suggested its ability to modify the bacterial composition of the tumor and, in turn, to modulate the immune function, thus affecting cancer progression and patient survival. Besides the possibility of formulating a prognosis based on the tumor microbiota, FMT results give us hope that one day we will be able to manipulate this microbiota to improve life expectancy of patients with PDAC, for whom very few therapeutic options are currently available.
Which bacteria live in your small intestine? Which colonize your colon? To learn all about the populations hosted in our gastrointestinal tract, swallowing a smart capsule packed full of high-tech could be enough.
To identify the bacteria living in our intestines, the method more frequently used consists in collecting stool samples. Although this technique has the indisputable advantage of being simple and non invasive, it also suffers from an obvious limitation: it only offers a residual insight into the gut microbiota but it does not give an account of the very different populations living throughout our gastrointestinal tract.
Targeted sampling
But things could very well change soon. In July 2019, an American team announced the development of a 3D printable capsule, that, once ingested, could find out everything about the gut microbiota, or more precisely, the different gut bacterial populations. Once a protective layer is dissolved in the small intestine, this encapsulated mini-laboratory takes bacteria samples surrounding it based on a system that does not require batteries. The capsule follows the same path as food, carried by natural intestinal movements, but thanks to a magnet it can be precisely placed in the specific region to be studied. To avoid losing this technological marvel “on its way out”, it is colored with a specific dye that turns fluorescent under a UV lamp..
Clinical trials should be soon conducted in humans
Of course, the capsule was thoroughly studied, first in test-tube experiments (in vitro) and later in pigs and primates (in vivo), in order to confirm it was able to identify the different bacterial populations in the various digestive segments, as well as their relative abundance. The only thing left to do is to carry out clinical trials to determine whether the capsule could also be used in humans for clinical purposes.
Understanding the distribution of the microbiota
“We learn more and more about the role of the gut microbiota on health and diseases”, explained Sameer Sonkusale, Professor of Electrical and Computer Engineering at Tufts University, and co-author of the study. “However, we know very little about its biogeography”, i.e. the distribution throughout the gastrointestinal tract. “This capsule will make it easier to understand the role of spatial distribution of bacterial populations within the gut microbiota in order to develop new therapeutic strategies.”
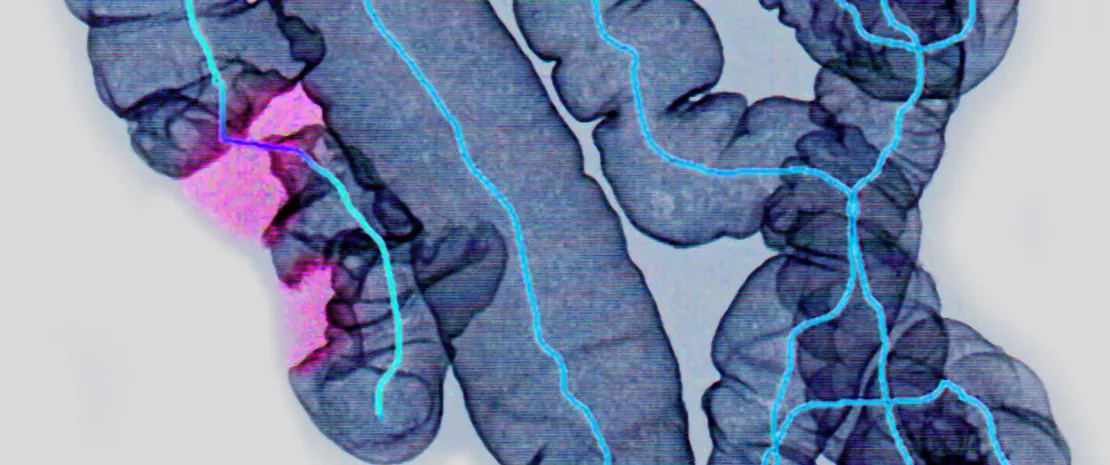
Using the gut microbiota to predict postoperative recurrence in Crohn’s disease: such is the possibility raised by a French study conducted in patients who underwent bowel resection.
While 50 to 75% of patients with Crohn’s disease will require at least one bowel resection during their lifetime, recurrence is observed in about 50% of them in the 5 years following their operation. Endoscopy is the gold-standard method to diagnose relapse. However, it can only be carried out a few months after the operation, thus delaying a potentially necessary early therapeutic intervention. The identification of early predictive factors of recurrence is thus of major interest.
Persistent dysbiosis
According to a multicenter study published in Gut and headed by Pr. Harry Sokol’s team, the microbiota present in the ileal mucosa could very well be one of these factors. To reach this conclusion, the researchers analyzed the composition of the microbiota extracted during bowel resection surgery (Tr), and later during follow-up endoscopy (Ts), in 201 patients. Result? Bowel resection caused a significant change in the microbiota in all patients and an improvement of the initial dysbiosis, but its effects were less pronounced in those who were relapsing. In the latter, between Tr and Ts, there was a decrease of alpha diversity, a more significant increase of several species from the Alphaproteobacteria class, and a lesser increase in some species from the Firmicutes phylum and the Lachnospiraceae and Ruminococcaceae families, which are believed to be markers of intestinal health.
Using the microbiota to predict recurrence
In modeling studies (some models take into account the factors modulating the recurrence risk: previous resection, tobacco use, male gender are aggravating factors while (sidenote:
anti-TNF
(Tumor Necrosis Factor) drugs are used to control inflammation.
) use is a protective factor), the researchers went further by identifying several taxa that are overabundant during the resection and that could be significant recurrence markers, especially bacteria from the Gammaproteobacteria class, Ruminococcus gnavus group and Corynebacterium genus. Despite some limitations, this study suggests that the composition of the microbiota at the time of bowel resection could predict recurrence and steer the postoperative therapeutic approach. There are however obstacles to the implementation of such an approach, especially the frequent preoperative use of antibiotics, which alter the microbiota and jeopardize its use as a predictive tool.
Parkinson’s disease might not only be due to neuron loss; it could also be impacted by the gut microbiota, our second brain. An Italian team tried to identify which bacteria might be involved.
Parkinson’s disease affects more than 1% of people over 60. It is the second most frequent neurodegenerative disease in the world. Previous studies have established a link between gut microbiota disruption ( (sidenote:
Dysbiosis
Generally defined as an alteration in the composition and function of the microbiota caused by a combination of environmental and individual-specific factors.
Levy M, Kolodziejczyk AA, Thaiss CA, et al. Dysbiosis and the immune system. Nat Rev Immunol. 2017;17(4):219-232.)) and the development of this disease through the gut-brain axis, but no definite conclusion has been reached regarding a specific bacterial composition associated to the disease.
Dysbiosis observed in patients with Parkinson’s
In recent studies conducted in 80 patients with several degrees of Parkinson’s, their gut microbiota was compared to that of 72 healthy persons.A dysbiosis was brought to light: the intestinal flora of patients displayed a higher abundance of bacterial species belonging to the Lactobacillaceae, Enterobacteriaceae and Enterococcaceae families, and a lower abundance of Lachnospiraceae. The more severe the disease was, the more apparent this difference as regards to Enterobacteriaceae and Lachnospiraceae, and the more important the motor disorders were. This is why researchers believed that these two bacterial families were correlated to the disease’s progression.
Neurotoxic inflammation
In the patients under investigation, the composition of the gut microbiota was affected by several parameters associated to the disease (duration, development stage, use of anti-Parkinson drugs), although they do not act on one specific bacterial family. The patients also displayed disrupted activity of neurotransmitters, i.e. molecules involved in mood regulation (serotonin, dopamine and norepinephrine); and they also produced more lipopolysaccharides, substances generating an inflammation that may damage neurons when they cross the intestinal barrier and the blood-brain barrier (that protects the brain from the surrounding blood). Although this scientific breakthrough is undeniable, it still needs to be further investigated (link between dysbiosis and gut inflammation, role of neurotransmitters in the gut-brain communication...).
Japanese researchers analyzed taxonomic and functional characteristics of the gut microbiota of patients who underwent a colonoscopy. Their results indicate that the flora is involved in the onset of colorectal cancer and experiences gradual changes as the disease progresses.
Tumor formations in colorectal cancer (CRC) is an extended process, which explains why clinical signs only appear at an advanced stage of the disease, although it is curable when treated early. The gut microbiota is strongly suspected to be involved in this process, based on both genomic and (sidenote:
Metabolomic
study of metabolites derived from the body or the environment and it takes place downstream from genomics (study of all genes), among others.
) data. Better understanding its role is thus important, from an etiologic and diagnostic perspective. That is why a Japanese team carried out metagenomic (N = 616) and metabolomic (N = 406) analyses on fecal samples from patients suffering from different stages of colorectal neoplasia and who underwent a colonoscopy. Patients were divided into nine groups: from the control group to CRC stage IV, through early stages such as multiple adenomatous polyps and intramucosal carcinoma (stage 0).
Changes in microbiota occurred from the early stages
Thanks to the advanced sequencing technique used (shotgun), the results revealed changes in the microbiota and the metabolome, not only in patients with advanced lesions but also at early stages. Two significant changes in the gut microbiota composition were observed during the development of CRC: on the one hand, a progressive increase in the relative abundance of some species (such as Fusobacterium nucleatum spp., Solobacterium moorei…), whichever the stage of the disease; and on the other hand, coexistence and increase of other species (such as Actinomyces odontolyticus), only in patients at an early stage. Moreover, increases in abundance of other species can characterize CRC progression, such as Parvimonas micra from stage I and Bilophila wadsworthia at stages III/IV.
The role of fecal bile acids confirmed
Significant differences at the metabolome level were also observed between groups that could be used to distinguish between healthy patients and those with a high risk of CRC. In patients with intramucosal carcinoma, significantly higher levels of branched chain amino acids (isoleucine, leucine and valine), phenylalanine, tyrosine and glycine were found. Bile acids, including deoxycholic acid, were significantly higher in all patients at an early disease stage, thus confirming the positive correlation already reported between fecal concentration of secondary deoxycholic bile acids and increased risk of CRC. All these results, obtained in a large cohort, show that changes happen in the gut microbiota as soon as warning signs of colorectal cancer appear, generating changes in fecal concentrations of some metabolites.
Staphylococcus aureus infections could be related to a greater risk of food allergies in young children with severe eczema, according to an international study that opens the way to the development of new approaches to prevent food allergies.
Staphylococcus aureus is a bacterium that is naturally present in the nose and skin of healthy people but is more abundant in children with eczema, especially when it is severe. This skin disorder is also a risk factor for developing food allergies. Thus, it could be easily imagined that the link between Staphylococcus aureus and food allergies in people with eczema is related to the severity of this disorder.
Multi-step study
This hypothesis was tested by a team of researchers using data collected during the (sidenote:
LEAP
Learning Early About Peanut Allergy
) study which monitored 640 children who were identified as high risk for peanut allergy (based on an existing egg allergy or severe eczema, or both) from early childhood to the age of 5. The results, published in 2015, had shown that preventing peanut allergy could be achieved, paradoxically, by introducing peanut to infants who are at high-risk for developing this allergy.
S. aureus, known culprit?
In this new part of the LEAP study, the analysis of the nose and skin microbiota of the children participating in the study showed that the more significant the Staphylococcus aureus colonization was, the more severe the eczema was and the more it worsened over time. The combination of these two disorders (Staphylococcus aureus infection + eczema), regardless of severity, is often associated with an increased production of molecules as part of the allergic reaction to peanuts, chicken egg white and milk. While it generally wanes with age, egg allergy persists in about 40% of children under study; and peanut allergy appears even in children who were preventively exposed from a very young age. The presence of Staphylococcus aureus in the nose or skin could thus lead to an allergic reaction to some diseases.
Towards a new potential therapeutic avenue
According to the researchers, S. aureus could prevent the development of a natural tolerance to eggs and peanuts, which would thus trigger the allergy. They thus suggested that eradicating S. aureus in children with eczema could prevent food allergies; and argue that further work should be carried out to elucidate the role of this bacterium in the development of these two disorders.
Olympia Tsilochristou, du Toit G, Sayer PH et al. Association of Staphylococcus aureus colonization with food allergy occurs independently of eczema severity. J Allergy Clin Immunol, 2019; doi.org/10.1016/j.jaci.2019.04.025
Professor Olivier Goulet is the Head of Gastroenterology, Hepatology and Nutrition at the Necker Children’s Hospital in Paris, France. His scientific approach focuses, among others, on the establishment of the intestinal microbiota from birth. Thanks to this research field it is possible to identify the parameters likely to modify or disrupt this early colonization and study its impact on the onset of certain pathologies.
GASTROINTESTINAL DISORDERS IN CHILDREN: THE NEED TO ACT
What are the main childhood gastrointestinal disorders involving the microbiota?
I count five of them. The first two are infectious (or post-infectious) diseases related to an infestation by pathogens, and inflammatory bowel diseases, which are due to a conflict between the immune system and commensal bacteria. But intestinal microbiota is also involved in food allergies, functional disorders (irritable bowel syndrome, constipation), as well as in obesity. Whether intestinal dysbioses are the cause or the consequence of these diseases has yet to be determined. Any change in the microbiota is likely to lead to functional changes, or even organic alterations, and conversely. Simply put, we estimate that infections can generate a dysbiosis and that chronic inflammatory bowel diseases can cause, as well as be caused by, a dysbiosis. The mechanisms involved in allergies are quite unclear but they could develop even before the maturation of the immune system, while later and/or prolonged changes could be involved in gastrointestinal functional disorders or obesity..
Is France especially exposed to this type of disease?
These observations are unquestionable, but they are not specific to France. The incidence of diseases mentioned earlier has increased in the past 20 years and I believe it could be called an “epidemic”. What changed? The number of C-sections, antibiotic administration and antacids. Our dietary habits and the composition of the food we eat, especially in terms of preservatives, also play a role. All these elements are involved in the disruption of our intestinal microbiota. We should not draw simplistic conclusions, but we should bear in mind that a wide range of arguments and studies correlate these changes to a significant increase in certain childhood diseases. The challenge is even more critical in pediatrics since events that happen at birth or early childhood tend to have a lasting impact on the microbiota composition and longterm consequences on health.
« We should adopt a true “culture of prevention” that includes the protection of intestinal microbiota. »
How can we improve this situation and improve patient treatment?
Health professional believe that the emergency is to obtain an easier and less expensive access to intestinal microbiota metagenomics analysis methods. This could provide a qualitative comparison of the microbiota composition of the same individual at different times. Identifying changes between “baseline microbiota” and that observed during the course of a disease could help us identify pathophysiological mechanisms and develop personalized or targeted therapeutic responses. In this context, the probiotics approach seems to be effective in certain intestinal disorders and deserves to be further investigated. Some countries are starting to show interest in this topic, but France must not be left behind, especially within the European Union. Moreover, we should adopt a true “culture of prevention”, with the support from public authorities, that includes the protection of intestinal microbiota. This would contribute to limit exposure to risk factors that are likely to generate dysbioses (C-sections, antibiotics, antacids, inadequate diet, etc.) and would decrease the number of several childhood diseases.
Persistent diarrhea is a major cause of child mortality but its origin remains controversial. The composition of the intestinal microbiota is a hypothesis which could lead to numerous answers regarding this disease with an unclear pathogenesis.
Persistent diarrhea is a particular form of the disease, defined as an episode lasting more than 14 days (beyond 30 days, it is called “chronic diarrhea”). The mortality rate attributed to persistent diarrhea has been determined (54% of all deaths caused by diarrhea) but its pathogenesis is still poorly understood: is it the progression of an acute episode or a disease in its own right? Through a literature review it was revealed that the majority of researchers consider persistent diarrhea to be an infectious disease associated to an intestinal colonization by pathogenic bacteria, be it followed by an acute or another episode.20 This colonization could be promoted by malnutrition and other factors (especially exposure to antibiotics) susceptible to cause intestinal dysbiosis.
... OR IS IT DUE TO MICROBIAL DYSBIOSIS?
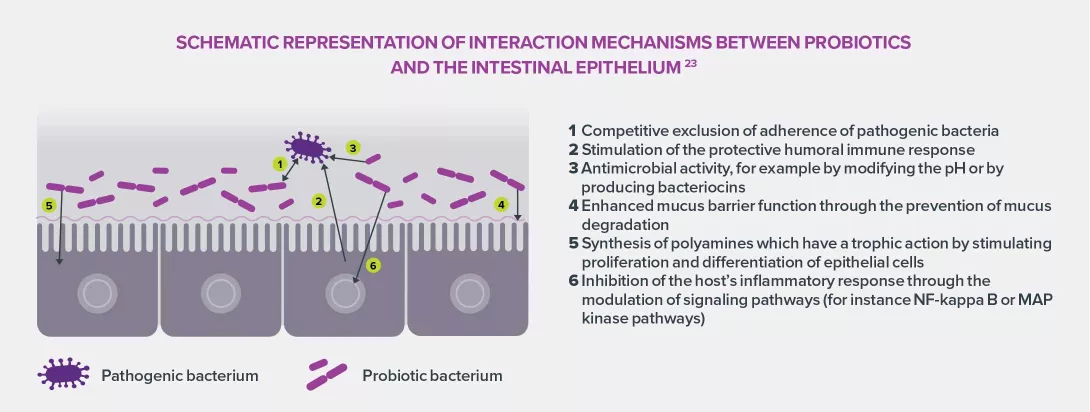
Among other etiologic hypotheses, the theory of a bacterial outbreak is gaining momentum. It was born from the observation that an abundant presence of commensal bacteria, especially Escherichia coli, disrupts lactose absorption. Connecting intestinal dysbiosis, levels of E. coli and persistent diarrhea could provide several clues to elucidate it pathogenesis. On this topic, certain probiotics have shown their efficacy to reduce the duration of acute diarrhea and persistent diarrhea in children.21, 22
Image
IDENTIFIED RISK FACTORS
An analysis of scientific literature provided a draft model of the disease pathogenesis. The first risk factor category includes very young age (under 1, risk x 3), malnutrition (risk x 2) and low birth weight (risk x 1.8). The second category includes an infection in the previous month (risk x 2) and a history of persistent diarrhea (risk x 3 to 6). The third category is related to eating habits (diet, breast milk substitutes...) which can multiply the risk by 4. Other factors have also been identified, including administration of antibiotics. Potential etiologies and confirmed risk factors underline the importance of a close collaboration between pediatricians, gastroenterologists, nutritionists and biologists. Interdisciplinarity could help obtain a deeper understanding of the relationships between infection, dietary habits and pathogenic and commensal microorganisms.
A close relationship has been established between childhood gastrointestinal disorders and intestinal microbiota. The composition of the intestinal microbiota impacts the risk of developing certain disorders, and conversely, a dysbiosis caused by a gastrointestinal disorder can play a role in promoting, worsening or increasing the recurrence of the underlying disorder. Research is focused on gaining a better knowledge of etiopathogenesis in order to develop new therapeutic and prophylactic solutions.
The fight against infectious diarrhea is a priority of healthcare systems in developing countries, since this pathology is the second cause of child mortality in these regions. Describing the intestinal microbiota and its dysbioses are part of this fight and could help offer personalized treatments.
RISKS ASSOCIATED TO DIARRHEA
Recurrent or prolonged diarrhea episodes increase the risk of malnutrition and stunted growth. They are also associated to numerous comorbidities: cognitive disorders, cardiovascular diseases, glucose intolerance, etc. Despite a regular decrease, near 525,000 children under 5 years of age die every year in the world. Understanding the etiology of diarrhea is a health priority, but the wide variety of types and potential causes requires further investigation, especially in terms of correlation with the intestinal microbiota. A recent study focused on Vietnamese population was added to the existing body of scientific literature on infectious diarrhea. It characterized the bacterial communities of 145 children with diarrhea and 54 controls.17
Image
ETIOLOGIC AGENTS WERE IDENTIFIED
Bacterial analysis of fecal samples revealed four major types of bacterial predominance in children with diarrhea: Bifidobacterium, Bacteroides, Streptococcus and Escherichia. The first two categories, usually asymptomatic, are close to the composition of the microbiota of control children. Predominance of Streptococcus and Escherichia in the microbiota of children who had the most severe symptoms, confirmed previous studies that associated these microorganisms with a higher risk of gastrointestinal disorders. Bacterial depletion was also observed in all categories. Nineteen taxa are concerned (mainly belonging to the Clostridiales and Erysipelotrichales orders) and especially Blautia hansenji which is known for its ability to produce SCFA19, essential to homeostasis.
INDIVIDUAL VULNERABILITIES
Age, nutritional status, intake of breast milk and etiology seem to contribute to the composition of bacterial communities during the early phase of diarrhea episodes. Streptococcus are more largely associated to young children (under 2) and bacterial infections, while Escherichia are found in older children and/or children with poor nutritional status. This extensive characterization is part of the analysis of the complex influences of infectious diarrheas on the intestinal microbiota and guides research towards new therapeutic approaches.
KEY FIGURES FOR DIARRHEA
Definition: passage of three or more loose or watery stools per day
Acute watery diarrhea lasting several hours or days
Watery and bloody diarrhea, or dysentery
Persistent diarrhea (14 or more consecutive days)
There are about 1.7 billion cases of diarrhea annually in children in the world.
2nd cause of death and major cause of malnutrition in children under.
525,000 deaths per year of children aged 5 or less in the world.
19 Short-chain fatty acids. They are products of carbohydrate fermentation (organic anions and saturated fatty acids) carried out by anaerobic bacteria in the colon
The severity of bronchiolitis in newborns may be assessed by characterizing their nasal microbiota. This could be an alternative, simpler and less invasive method than a nasopharyngeal aspirate, which is conventionally used.
As is the case for bronchiolitis, characterization of the airway microbiota takes on a particular importance in some pulmonary pathologies. The severity of the disease is direct y correlated with the local microbial populations. Consequently, accurate identification of the microorganisms present proves essential and requires high-quality sampling. Standard protocol (nasopharyngeal aspirate) of fers good diagnostic and prognostic efficacy. But the procedure is invasive and proves tricky to perform in children, in particular in infants. Simpler to perform and less traumatic, nasal swab is a promising alternative. Its efficacy was studied by comparing the nasopharyngeal and nasal microbiota of infants with bronchiolitis (composition / capacity to predict the severity of the inflammatory episode).16 Both sampling techniques were assessed in 815 hospitalized children; bacterial populations were characterized by amplification of 16S rRNA genes.
DIFFERENT POPULATIONS, BUT SIMILAR PREDICTABILITY
The analyses show a disparity between the microbial populations of the two areas. The nasal microbiota is composed mainly of the genera Staphylococcus (40.8%), Corynebacterium (10.4%), Moraxella (9.3%), Haemophilus (7.4%), Dolosigranulum (5.2%), Streptococcus (5%) and Enterobacter (4.7%). However, the nasopharyngeal microbiota is dominated by the genera Moraxella (30.7%), Streptococcus (30.5%) and Haemophilus (19.7%). These differences however should be put in perspective: predominance of Moraxella or Haemophilus in the nasal area is also found in the nasopharynx, making these two sites a good tool for predicting the severity of bronchiolitis. Children with a Haemophilus-dominant profile display an increased risk of requiring intensive care or prolonged hospitalization (≥ 5 days). In comparison, subjects with a Moraxella-dominant profile seem to be the least at risk. This predictive capacity is not however applicable to other bacterial genera. The nasal swab presents many practical advantages, and can therefore be considered a valid alternative to nasopharyngeal aspirate in assessing the severity of bronchiolitis in infants.