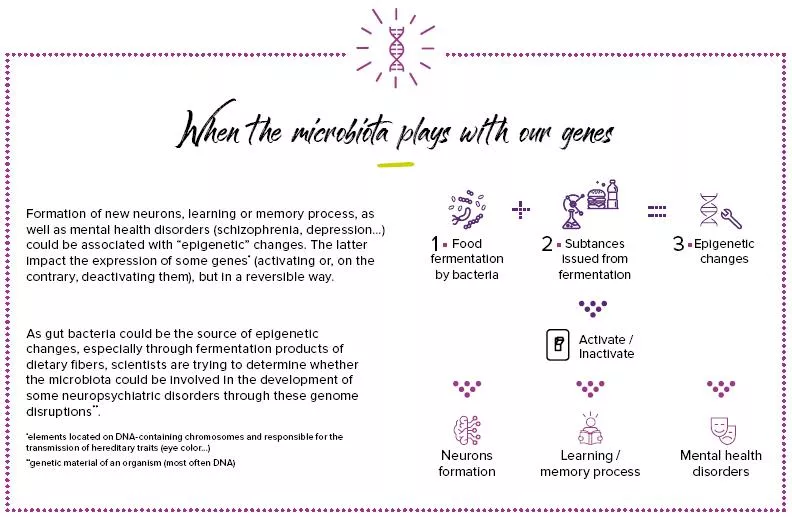
Microbiota and Autism spectrum disorders
Microbiota disruptions in the first years of life, when our intestinal flora and brain are developing, can affect brain structures and functions and promote developmental disorders. Autism spectrum disorders (ASD) include a number of contrasted disorders8 associated to brain development defects. They could be related to a microbiota disruption induced by pregnancy and during the first few years of life: some gastrointestinal signs, frequently associated to this disorder, led scientists to believe that the microbiota was undoubtedly a way of understanding autism spectrum disorders.
The gut microbiota
Symptoms appear early in life and include communication deficit, social communication and behavior disorders as well as repetitive behaviors. Compared to the general population, affected people are more subject to gastrointestinal disorders (diarrhea, abdominal pain, constipation), whose severity seems sometimes related to that of the disease’s symptoms.
Microbial “signatures”?
Autistic children seem to have a less diversified flora than other children: it has lower contents of bacteria known to be beneficial such as Bifidobacterium, and higher contents of others (Lactobacillus, Clostridium…). Moreover, autistic children intestines seem to host more Candida (especially Candida albicans) than usual. But this fungus produces ammoniac and toxins that can impact the brain’s functioning and exacerbate intestinal bacterial disorders.
Several risk factors
In animals, a high-fat maternal diet during pregnancy could be associated to an imbalance of the gut microbiota–called “dysbiosis”–and the onset of autistic disorders in their offspring. Children born through C-section who received many antibiotics also seem to have a higher risk of developing these disorders. The upside is that breastfeeding during the first 6 months of life (minimum) could decrease the risk of developing these disorders at a later age.
OPEN WIDE AND SAY “AH”: THE NEW DIAGNOSTIC TEST FOR AUTISM?
- Current screening is based on behavioral, psychomotor, psychological and language signs. It is possible to establish a diagnosis as early as the age of 2, but diagnostic delay is frequent.
- A recently developed 96%-accurate mathematical algorithm seems to be very promising and could be added to the diagnostic arsenal: it was tested on 32 affected children and could help detect new autism9 biomarkers (exceeding amounts of “bad” bacteria” and decreased diversity) in the oral flora (saliva and dental plaque).
Microbiota: a therapeutic hope?
A few avenues are under investigation: probiotics for instance, which could improve gastrointestinal disorders and relieve autistic symptoms, similarly to some antibiotics. Despite a significant infectious risk, fecal transplant10 could also be useful to reduce autistic behaviors and associated gastrointestinal disorders7 in children and adolescents. Finally, diet is of great interest. The use of omega-3 supplements could improve behavior: a diet free of gluten or milk proteins as well as a high-fat low-carb diet (called “ketogenic”) could increase sociability as well as the ability to communicate and decrease stereotyped behaviors.
7 Sharon G et al. The Central Nervous System and the Gut Microbiome. Cell. 2016 Nov 3
8 Li Q, et al. The Gut Microbiota and Autism Spectrum Disorders. Front Cell Neurosci. 2017
9 Qiao Y, Wu M, Feng Y, et al. Alterations of oral microbiota distinguish children with autism spectrum disorders from healthy controls. Scientific Reports, 2018
10 Fecal transplant from healthy donor(s) aimed at restoring the balance of microorganisms in the recipient patient
11 Cenit MC, Nuevo IC, Codoñer-Franch P, et al. Gut microbiota and attention deficit hyperactivity disorder: new perspectives for a challenging condition Eur Child Adolesc Psychiatry (2017)
12 Cenit MC, et al. Gut microbiota and attention deficit hyperactivity disorder: new perspectives for a challenging condition. Eur Child Adolesc Psychiatry. 2017 Sep.
13 Lange K. Dietary factors in the etiology and therapy of attention deficit/hyperactivity disorder. Current Opinion in Clinical Nutrition and Metabolic Care. (2017)