Dampening gastrointestinal inflammation through nutrition
by Dr Genelle Healey

There are many ways to influence gut microbiota composition and modulate the immune response (prebiotics, probiotics…).31 One of the options is dietary interventions that have the potential to alter the activity of the local immune system, thereby dampening the increased inflammatory tone observed with these conditions - this is termed immunonutrition.32 The most widely studied immunonutrients include omega-3 polyunsaturated fatty acids (n-3 PUFA), vitamin D, arginine, nucleotides and glutamine.32
Vitamin D and its effects on intestinal immune responses
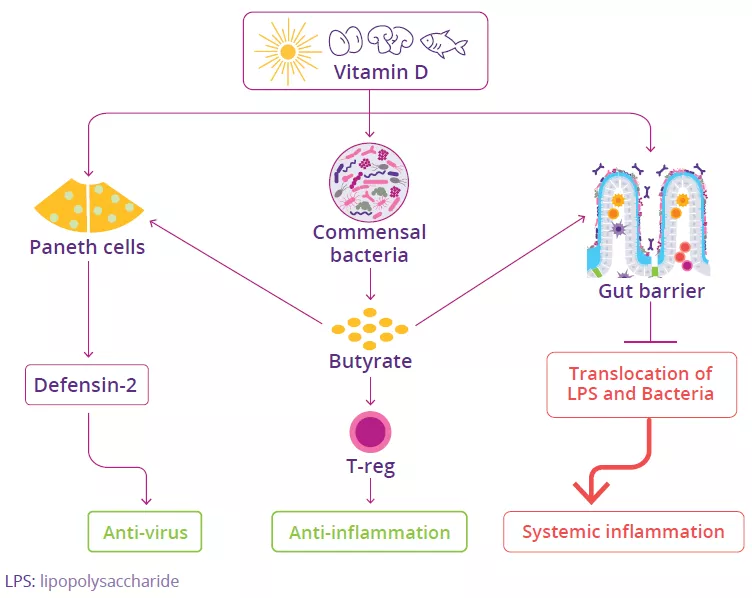
While the best characterized function of vitamin D is its role in controlling calcium levels and thereby maintain bone health, it is also known to have a significant effect on GI immune responses. Vitamin D regulates several genes that regulate gut barrier function as well as genes that encode antimicrobial peptides, thus helping to maintain intestinal balance (Fig 5).33 It exerts an immunomodulatory effect, including immune cell differentiation, migration and anti-inflammatory functions,34 and can act directly on Paneth cells to promote defensin-2 secretion.35 Vitamin D also promotes the compositional diversity of the gut microbiota, leading to increased production of butyrate. Butyrate can exert anti-inflammatory effects, increase gut barrier function, and promote Paneth cells to secrete defensins (Fig 5). Interestingly, some probiotic bacteria (e.g. Lactobacillus strains) have been shown to increase vitamin D levels in the blood.36
FIGURE 5: Effects of vitamin D on intestinal cells, gut microbiota and gut barrier.
Adapted from Chen J et al, 2021.37
38 Roseland JM, Phillips KM, Patterson KY, et al. Vitamin D in foods: An evolution of knowledge. Pages 41-78 in Feldman D, Pike JW, et al, eds. Vitamin D, Vol 2: Health, Disease and Therapeutics, 4th Ed. Elsevier, 2018.