Comments on the original article of Chen et al. (N Engl J Med 2020) [1]
Environmental enteric dysfunction (EED) is an enigmatic disorder of the small intestine that is postulated to play a role in childhood undernutrition, a pressing global health problem. Defining the incidence of this disorder has been hampered by the difficulty in directly sampling the small intestine mucosa and the microbiota. This study involved 110 young children exhibiting linear growth stunting who lived in an urban slum in Bangladesh, and who had not benefitted from nutritional intervention. The authors performed an endoscopy on 80 children who had biopsyconfirmed EED and for whom samples of plasma and duodenum were available. Of the bacterial strains obtained from the children, the absolute levels of a shared group of 14 taxa (not typically classified as enteropathogens) were negatively correlated with linear growth and positively correlated with duodenal proteins implicated in immuno-inflammatory responses. The representation of these 14 duodenal taxa in the faecal microbiota was significantly different from that of samples obtained from healthy children. Enteropathy of the small intestine developed in gnotobiotic mice that had been colonised with cultured duodenal strains obtained from children with EED. These results confirm the existence of a relationship between delayed growth and components of the microbiota of the small intestine and enteropathy, and provide a rationale for the development of therapies targeting these microbial contributions to EED.
WHAT DO WE ALREADY KNOW ABOUT THIS SUBJECT?
The proportion of chronic undernourishment with growth stunting is 25 % in infants who have had more than 5 episodes of diarrhoea. These recurrent intestinal infections result in EED, a disorder characterised by villous atrophy combining a reduction in intestinal surface area and absorption capacities, alteration of the intestinal barrier and mucosal inflammation. More recent data suggest that microbiota dysbiosis of the upper gastrointestinal tract may be present in EED.
WHAT ARE THE MAIN INSIGHTS FROM THIS STUDY?
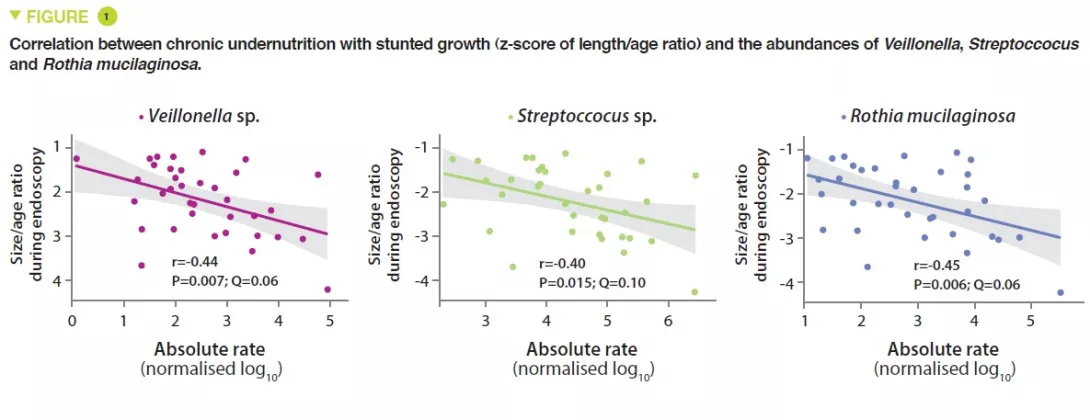
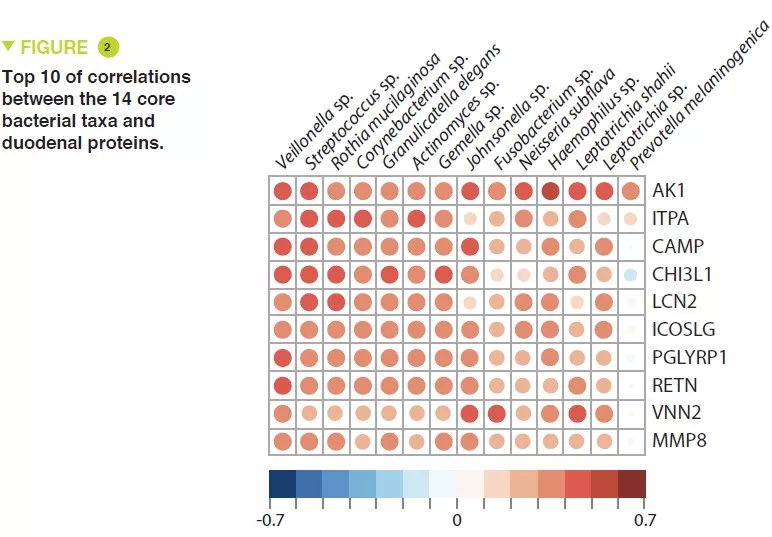
This study included 110 infants with a mean age of 18 months, from Dhaka, Bangladesh, who had chronic undernutrition with stunted growth, defined by nutritional intervention. Duodenal biopsies confirmed the presence of EED in 80 of them. The duodenal aspirate microbiota from 36 of these infants was analysed; a group of 14 bacterial taxa was present in over 80% of this population and were negatively correlated with the length/age ratio (r = – 0.049, p = 0.003) (Figure 1). The proteomics study of the duodenal biopsies showed a positive correlation between these 14 taxa and 10 proteins including 2 antimicrobial peptides, a marker of intestinal inflammation (LCN2), and a negative correlation with 10 proteins produced by the enterocytes (Figure 2).
In the 80 infants with demonstrated EED, the plasma proteomics study showed a strong positive correlation with REG3A and LCN2.
Comparison of the faecal microbiota of EED infants with 27 controls revealed a significant increase in Veillonella genus bacteria which were the most highly correlated with the duodenal proteins implicated in gastrointestinal inflammation.
After culture of 39 bacterial strains from duodenal aspirates of infants with environmental enteric dysfunction, including 11 of the 14 taxa, these were administered by oral gavage to mice that had been fed a diet similar to that of an 18-month-old Dhaka infant. Twenty-three of these bacteria were found to be present with a relative abundance > 0.1% in at least one part of the gut. Control mice received the caecal microbiota of conventionally raised mice by oral gavage. In contrast to the control mice, mice receiving “environmental enteric dysfunction” bacteria, exhibited infiltration of inflammatory mononuclear cells in the lamina propria of the small intestine in addition to epithelial abnormalities and architectural distortion with elongated crypts. These abnormalities had a patchy location in the small intestine but did not extend to the colon.
From a functional viewpoint, the results showed in these mice an increase in mRNA expression of anti-microbial peptides (Reg3b and Reg3g), an increase in a metalloproteinase (MMP8) and a reduction in mRNA encoding tight junction proteins. These alterations in the innate immune response and of the mucosal epithelial barrier may explain the systemic bacterial translocation to the spleen (Escherichia coli and Enteroccocus hirae).
Image
Image
Key points
Environmental enteric dysfunction is promoted by a disturbance in the intestinal microbiota at the duodenal level
This duodenal dysbiosis is correlated with chronic undernutrition
The pathology is transmissible to mice, which could help understanding the physiopathological mechanisms involved (intestinal inflammation, abnormalities of the epithelial barrier and immune alterations of bacterial signalling)
Conclusion
The results of this study suggest a causal relationship between the bacteria of the duodenum, environmental enteric dysfunction and chronic undernutrition with stunted growth. It is suggested that these children could therefore benefit from the development of treatments targeting this dysbiosis.
Commentary on the original article by Mars et al. Cell 2020 [1]
The gut microbiome is implicated in numerous chronic gastro-int estinal disorders in humans. Determining its role however has been rendered difficult due to the lack of correlation between animal and human studies as well as that of an integrated multi-omics view of disease-specific physiological changes. The authors integrated longitudinal multi-omics data from the intestinal microbiome, the metabolome, the host epigenome and the transcriptome in the context of irritable bowel syndrome (IBS) host physiology. They have identified IBS sub-type specific and symptom-related variations in microbial composition and function. A sub-group of changes identified in microbial metabolites corre sponds to host physiological mechanisms which are relevant to IBS. By compiling multiple data layers, the authors identified purine metabolism to be a new host-micro biota metabolic pathway in IBS with potential for therapeutic application. This study highlights the value of longitudinal sampling and the integration of complementary multi-omics data in the identification of functional mechanisms which may be future therapeutic targets in a global treatment strategy for chronic intestinal diseases.
WHAT DO WE ALREADY KNOW ABOUT THIS SUBJECT?
Irritable bowel syndrome (IBS) is a disorder observed in patients all over the world, characterised by recurrent abdominal pain or discomfort. Occurring mainly in women, IBS is associated with changes in the form or frequency of stools and it is the form of the latter which defines the IBS subsets: IBS with constipation (IBS-C), IBS with diarrhoea (IBS-D) or IBS with mixed bowel habits (IBS-M).
The pathogenesis of IBS involves changes in gastro-intestinal motility, intestinal secretion, visceral hypersensitivity and intestinal permeability, all of which can be modified by the gut microbiome [2]. Moreover, IBS symptoms are influenced by the diet, host genetics and the environment, which are also known to modulate the human gut microbiome [2]. Experimental evidence supporting the role of the gut microbiome in IBS are based on patient-to-gnotobiotic mouse transplantation studies which reproduced certain symptoms associated with IBS-C and IBS-D (transit time, sensation of pain, intestinal permeability…) [3]. However, in the absence of robust animal models of IBS, studies in humans are needed to determine the interactions between the gut microbiome and the pathological pathways specific to humans. Human IBS studies are limited in general by the use of transversal sampling and a failure to stratify into patient subsets, which is reflected in the lack of agreement in the results obtained in the large number of studies on the microbiome [4].
The well-described influence of gastro-intestinal transit on the intestinal microbiome increases the variability of the studies even more. In addition, IBS, in common with other chronic gastro-intestinal disorders, is characterised by periods of remission and flare up of the symptoms, and transversal sampling therefore fails to take into account the fluctuations of the disease over time. Lastly, the inherent differences in host physiology between humans and animals have been an obstacle to progress in our understanding of the mechanistic roles of the gut microbiome in IBS. The authors performed a longitudinal study in subsets of patients with IBS, integrating multi-omics measurements, including the microbial metagenome, host transcriptome and the methylome with assessment of host cell functions. This revealed mechanisms specific to the IBS subset induced by impaired microbial metabolism, which corresponded to simultaneous changes in the host physiology.
Key point
The functions of the gut microbiota are impaired in IBS and there are differences between IBS-C and IBS-D
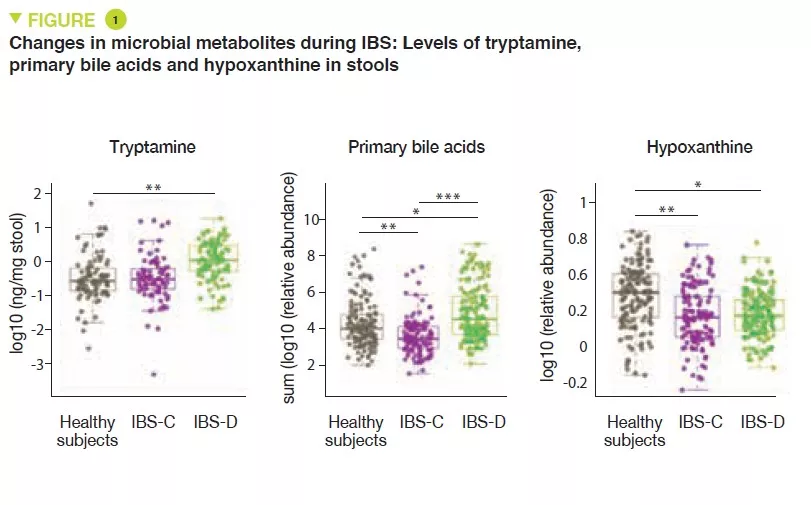
The increase in the production of tryptamine and the reduction in transformation of bile acids may be implicated in IBS-D
Over-consumption of hypoxanthine by the microbiota and host cells may be implicated in IBS by altering the energy level of the intestinal mucosal epithelium cells.
Image
WHAT ARE THE MAIN INSIGHTS FROM THIS STUDY?
Here, the authors conducted a prospective observational longitudinal study with multi-omics analysis of the gut microbiome and the host cells. Healthy subjects were compared with patients with IBS-C and IBS-D. A total of 77 participants supplied at least one stool sample (a total of 474 stool samples were obtained), and 42 participants received a sigmoidoscopy which provided colon biopsies. In order to identify the microbial factors causing the symptoms specific to each of the IBS subsets, metagenomic sequencing and a metabolomic analysis were performed on the stool samples. A metabolomic analysis and cytokine assays were performed on serum samples. Lastly, 16S sequencing, and metabolomic, transcriptomic and methylomic analyses were performed on the colon biopsies. The authors identified differences in the composition and diversity of the gut microbiota between healthy subjects and IBS-C or IBS-D patients.
Metabolomic analysis of the stools revealed increased levels of tryptamine, a tryptophan metabolite produced by certain intestinal bacteria, in patients with IBS-D (Figure 1). Because tryptamine accelerates transit due to an action on the serotonin receptor, 5-HT4, it is suggested that it could have a role in the phenotype of these patients. Similarly, the proportion of primary bile acids was higher in patients with IBS-D, a sign of impaired transformation of bile acids by the microbiota. In vitro experiments suggest that primary bile acids increase secretion in the colon and could also participate in the phenotype.
Lastly, the integration of multi-omics data identified a potential new mechanism in IBS. The results suggest that in IBS patients there is increased degradation of purine nucleotides and of hypoxanthine in particular, by the microbiota and the host cells, which induces stress in the colon. It is suggested that this could lead to a compensatory response with an increase in purine recuperation. The low levels of purine nucleotides could lead to a reduced source of energy to the mucosal epithelium and to a reduced capacity for repair of the gut mucosa, which could partly contribute to IBS physiopathology.
WHAT ARE THE CONSEQUENCES IN PRACTICE?
These data suggest a role of the gut microbiota in the physiopathology of IBS with differences between IBS-C and IBS-D. Moreover, these results point towards the potential role of a deficiency in purine nucleotides, in particular via an over-consumption of hypoxanthine by the microbiota and the host cells. These results point the way to treatments stimulating the production of microbial hypoxanthine or inhibiting xanthine oxidase locally in the intestine.
Conclusion
This longitudinal study with integrated multi-omics shows the value of longitudinal studies in humans and highlights functional alterations to the microbiota in IBS which may potentially be implicated in the physiopathology of this disease. The new leads which have been identified may be new therapeutic targets.
Probiotics: essential information for understanding and choosing them correctly.
What exactly are probiotics? They were not “officially” defined until the 21st century. However, consumption of these beneficial microorganisms goes back to time immemorial.
Did you know? Our ancestors took the ancestors of today’s probiotics!1 From Neolithic times, fermentation of certain foods has been seen to hold incredible virtues. Milk, wheat, or vegetables became easier to preserve, tastier, easier to digest… and better for health.1,2
From the beginnings of time, at least 5000 years ago, the Egyptians, Romans and Hindus already appreciated fermented milk,2 and the Turks considered it to be the elixir of life. Is it the secret to their legendary strength? Three centuries before our era, Chinese workmen building the Great Wall of China ate fermented cabbage to keep healthy.2 The famous Hippocrates, “father of medicine” recommended that Olympic athletes eat cheese.1 Even the soldiers of the terrifying Genghis Khan found fermented milk to be a source of vigor that allowed him to win battles!3 But it was not until the beginning of the 20th century, particularly after Louis Pasteur’s work, that we discovered that these virtues were due to beneficial microorganisms.1
What is a probiotic?
Probiotics are “live microorganisms which when administered in adequate amounts confer a health benefit on the host”. 4,5
Do you need explanations for this original expert version?
Live...
On good form, ready to act: dead microorganisms are not probiotics!
microorganisms…
Like bacteria or yeasts.
which when administered in adequate amounts…
Just the right amount to act effectively and safely.
confer a health benefit on the host.
In this case, they have a positive effect on the health of the person taking them.6
A probiotic is not…
… an antibiotic, quite the contrary! The term “probiotic” (for life) was suggested by researchers in the 1960s, as opposed to “antibiotic” (against life).1
… a microbiota, which describes all the microorganisms present in a given environment - such as the gut. The microbiome, is simply the genome (all the genes) of all these microorganisms!7
… a prebiotic, consists of special, non-digestible food fibers that specifically nourish the good bacteria in the microbiota and, thereby, are beneficial for health.8 When they are added to probiotics in specific products, they are called symbiotics.9
… a fermented food, which is a food that has been elaborated with certain living microorganisms and via certain enzymatic transformations—such as yogurt, cheese, fermented cabbage—is not necessarily a probiotic even though it has health benefits.10
… fecal microbiota transplantation (FMT) is a treatment consisting of treating the microbiota of a sick person by transplanting that of a healthy donor. Currently, FMT is only used in cases of relapsing intestinal infections caused by a bacterium called “Clostridioides difficile”.11
What are probiotic microorganisms?
Commonly called “microbes” or even “germs”, microorganisms are “microscopic” living beings, that means that they cannot be seen by the naked eye.12 They often consist of only one cell!
Microorganisms include bacteria, which are ubiquitous in our environment: they can be found in the earth, water, and even on and in our bodies!12, 13 Microscopic fungi can also be found: yeasts (from Saccharomyces, the baker’s yeast, to Candida, which causes fungal infections) or molds (like Penicillium, which gives Roquefort cheese its “blue” color, but also penicillin, the famous antibiotic).12,14,15,16 Viruses are also microorganisms, but as they cannot survive without infecting a cell, they are still not considered as “living beings”.12,17 There are also amoeba, microalgae, etc.18,19 This little world is actually gigantic: there is already a billion bacteria in a teaspoon of earth! But fear not! Over 99% of them are harmless for humans.12,20
The microorganisms that are most commonly used as probiotics are:
yeasts, such as Saccharomyces boulardii, isolated from the skin of lychees.3,15
All are designated by a specific Latin name
Their genus comes first, for example Lactobacillus,
followed by the species within the genus, which gives for example Lactobacillus “acidophilus”,
and finally, the strain contained within this species, in the form of a series of letters and/or numbers, which like a barcode indicates and precisely identifies the microorganism. The strain differentiates the genetic particulars of each species of microorganism, making each probiotic unique.21
For example, Lactobacillus acidophilus XYZ123
Have you forgotten your Latin?
Think of a fruit salad with plums, cherries, peaches and nectarines. They all come from the same genus of tree, the Prunus. For example, the species Prunus avium gives cherries, while Prunus persica gives peaches - of which there are even more varieties: yellow, white, smooth or fuzzy, round or flat, etc.22
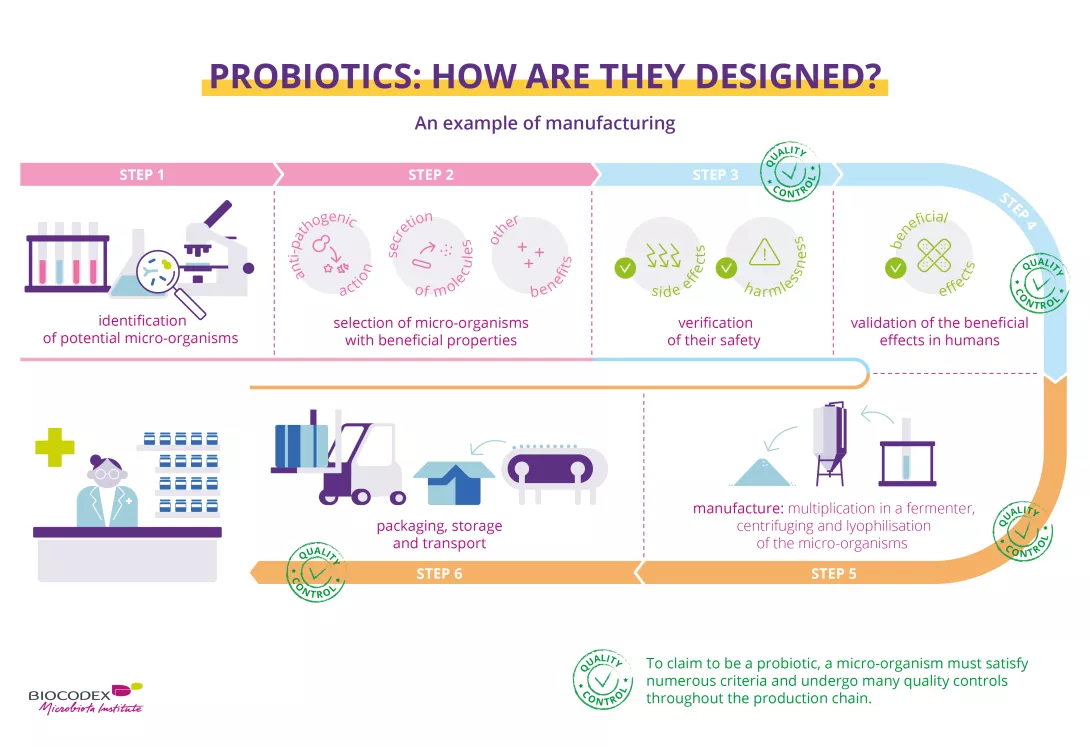
How are probiotics chosen?
Finding the “chosen ones” among the billions of species of microorganisms: that is the hard task that researchers face! Probiotic species often bear the names of their researchers, to commend their efforts: Saccharomyces boulardii was isolated by Henri Boulard23 and Lactobacillus reuterii (which is now called Limosilactobacillus reuteri24) by Gerhard Reuter25.
Regardless of whether they come from milk, fruit, or the human body, potentially beneficial microorganism species are studied from every conceivable angle in order to find the most promising strains.
The first stage consists in identifying them, following the characteristics of their genome. The microorganisms are classified. They are given a name and a strain number.4,26
The second stage consists in gradually reducing the potential candidates on the basis of their beneficial properties, such as anti-pathogenic, anti-cholesterol, or bowel-regulating actions.4,26
The third stage consists in verifying their safety, i.e., whether there are any health risks; researchers therefore check whether they contain antibiotic-resistant genes, toxins, and whether they cause any undesirable effects. They also check whether the candidate probiotics are capable of surviving in certain extreme conditions, such as the gut (temperature, pH, bile acids, etc.).4,26
The fourth stage is not to be taken light-heartedly. It is when the efficacy of the probiotic is validated in humans, in what are called “clinical trials”, which should follow precise recommendations from the local or national health care authorities. It is at this stage that the tested microorganism can be classified as a probiotic.4,26
In the last stage, researchers ensure that the probiotic is alive and remains at the effective dose throughout the product’s shelf-life. The probiotics are then stored in an “international microbial strain bank”.4,26
What are probiotics for?
Our bodies contain several microbiota. The most important one is in the gut (that is, the “intestinal flora”), but there is also a microbiota of the skin, the vagina, the mouth, the respiratory tract, etc.28,29 Billions of microorganisms work together within these microbiota.28,30 The majority is harmless or beneficial for health.31 Some are potentially pathogenic; in other words, they could cause diseases, but their development is impeded by “friendly” microorganisms32. For different reasons, such as unhealthy eating, stress, disease, or a course of antibiotics, the equilibrium of the microbiota can be disrupted. This is called “ (sidenote:
Dysbiosis
Generally defined as an alteration in the composition and function of the microbiota caused by a combination of environmental and individual-specific factors.
Levy M, Kolodziejczyk AA, Thaiss CA, et al. Dysbiosis and the immune system. Nat Rev Immunol. 2017;17(4):219-232.)”.28,30 The composition of the microbiota is changed; it becomes weaker, beneficial microorganisms are less abundant, and pathogens seize the opportunity to colonize the space and multiply…33
By reinforcing the microbiota, probiotics can help it to maintain or regain its equilibrium, acting on our immune defense system by reducing inflammation, protecting us by attacking (sidenote:
Pathogen
A pathogen is a microorganism that causes, or may cause, disease.
Pirofski LA, Casadevall A. Q and A: What is a pathogen? A question that begs the point. BMC Biol. 2012 Jan 31;10:6.) or their toxins. They thus prevent or correct the disorders or diseases associated with dysbiosis.34,35,34 Nonetheless, depending on the strain, probiotics have different modes of action, and a specific beneficial effect may not be extrapolated from one strain to another.37
Why take probiotics? What are the benefits? What is in it for me?
Probiotics have several benefits for our health. However, according to the efficacy that each probiotic strain has shown in studies conducted on humans, they have proven their worth in very specific situations.5,38
Digestive system disorders, such as antibiotic-associated diarrhea,39C. difficile diarrhea,40gastroenteritis,41traveler’s diarrhea,42 functional bowel disorders (or “irritable bowel”),43,44 lactose digestion disorders,21 inflammatory bowel diseases (IBDS)45 etc
Probiotics are manufactured using a delicate technical process with strict quality controls at every stage of the production line. In fact, they must be produced in a way that guarantees the end product meets all quality and safety standards. The probiotic micro-organisms must stay alive, in a sufficient number and stable until the end of the product’s shelf life, be in the correct dose to produce the stated benefits, and be free from contaminants.5,6,51
This infographic is a simplified and non-exhaustive illustration of the process for selecting and manufacturing probiotics with theoretical examples of quality controls.
Stages of manufacture6,52
This step-by-step process is a simplified and non-exhaustive illustration of the process for manufacturing probiotics.
Culture
The chosen micro-organism is cultured with sterilized nutritional substances to encourage it to multiply.
After they have multiplied, the micro-organisms are separated from the culture medium using centrifugation or filtration.
Lyophilization
The resulting paste then undergoes fast freezing followed by dehydration to extract any water; this is known as lyophilization, which evaporates at least 96%53 of the remaining moisture. This preserves the micro-organisms whilst ensuring they stay alive.
The powder is then packaged in its final form (hard capsules, sachets, ampoules, etc.). The choice and quality of formulation will increase the stability of the product. They are then packaged in their outer container or box.
Storage
The packaged probiotics are stored in controlled conditions (e.g., temperature, humidity, etc.).
Delivery
The batches are then delivered to their point of sale, e.g., a pharmacy.
At each stage of the manufacturing process - even sometimes at several points during a single stage - samples are taken and analyzed to ensure that the product is compliant, in other words to check for optimal quality and purity.6 The micro-organisms must still be alive and safe to consume.6 So that consumers can have complete faith in the quality of their products, some laboratories use not only internal checks but external independent assessors to ensure that the entire manufacturing and quality control process complies with regulations and best practice.27
Choosing the right probiotic among so many is not always easy, as you can see. Not all probiotics are the same. And no probiotic strain or combination of strains will have all of the beneficial effects reported here at the same time.50 Ask your doctor or pharmacist for advice; they will recommend the right products based on your health condition.
There has been a lot of research into human microbiota and probiotics over the past several years. Driven by technological advances in biology, it provides us with new and sometimes surprising scientific insights into the subtle and complex interactions within microbial ecosystems. For precision probiotics, microRNAs, probiotic consortia, postbiotics, etc., research is paving the way for new and promising proposals to meet the current and future health needs of us all.
Science has already revealed some of the secrets behind how probiotics affect our health. We now know that the beneficial effect of a probiotic depends both on the strain and on certain characteristics of the individual consuming it, such as age, diet, state of health, medication and microbiota. 54 As a consequence, this effect can vary between individuals. 55 In recent years, major scientific advances have been made in understanding the interactions between microbiota and the human body. They suggest that modulating these microbial ecosystems could provide new solutions to major nutritional and health issues. 56
So how can we ensure that future probiotics are more effective, more targeted and better adapted to each individual's microbiota? Many teams of scientists have already delved into this vast field of research. The tools they use to gain a better understanding include:
The scientific knowledge provided by these new methods has enabled researchers to gain a much more detailed understanding of the organization of the microbiota, namely how it works, how the microorganisms interact with each other and with the individual that harbors them, etc. 56 What is the goal? To identify the microorganisms that are key to its balance. In doing this, researchers are able to isolate specific strains and target them for their potential benefits for the microbiota and health. They can also observe the mode of action of these future probiotics within their cells, their interactions with the microbiota and the host's response 54, 57.
Next generation probiotics
These new scientific and technological approaches have led to the emergence of what is referred to as (sidenote:
Next Generation Probiotics (NGP)
Live microorganisms identified based on comparative analyses of the microbiota which confer a health benefit to the host, when administered in adequate amounts.
Martín R, Langella P. Emerging Health Concepts in the Probiotics Field: Streamlining the Definitions.Front Microbiol. 2019;10:1047.). Among the most recently identified are Roseburia intestinalis, Faecalibacterium prausnitzii, Akkermansia muciniphila. These strains, which come from species that are key for the human microbiota, are thought to act on physiological processes (metabolism, immunity) that are not necessarily affected by conventional probiotics 56 and on certain specific pathological mechanisms involved, for example, in cancer, obesity, diabetes, cardiovascular, inflammatory and auto-immune diseases, pain, etc. 56,58,59,60 They could therefore be classified as (sidenote:
Live Biotherapeutic Product (LBP)
Biological product containing living microorganisms, such as bacteria, and intended to prevent or treat disorders and diseases (vaccines do not fall into this category).
Rouanet A, Bolca S, Bru A, et al. Live Biotherapeutic Products, A Road Map for Safety Assessment. Front Med (Lausanne). 2020;7:237.
), i.e., medicinal products containing live organisms . Next generation probiotics primarily refer to those strains which do not have the history of use as probiotics. But they may also be previously known probiotics that are genetically modified to produce specific molecules of interest, such as short-chain fatty acids (SCFAs), to increase their survival in the digestive tract and improve their metabolism, immunomodulatory properties, ability to fight certain pathogens, etc. 60
Precision probiotics for personalized medicine
The days of "precision probiotics” are already upon us. And by taking advantage of the variability of the host response, the era of personalized probiotics is dawning! As the concept of personalized medicine is based on factoring in the specific characteristics of each patient in order to overcome the disease, "next generation" probiotics can naturally be integrated into this approach due to their ability to modulate the host microbiota depending on its characteristics. 54 Researchers are now devising ways of analyzing the gut microbiota of anyone who might benefit from a probiotic in order to determine the most suitable one beforehand. The development of miniaturized devices that can be ingested and take a flora sample in order to characterize it is already being considered. Scientists also believe that thanks to the democratization of high-speed sequencing, each of us could soon have access to the genome of our microbiota and thus be able to obtain personalized recommendations for staying in good health through nutrition, probiotics or prebiotics. 54
New public health applications
Probiotics are currently being considered as a response to public health issues, particularly in situations where conventional therapeutic options are lacking. For example, in light of the worrying increase in antibiotic resistance worldwide, probiotics with antimicrobial or immunomodulatory activity are being studied as alternatives to antibiotics. The therapeutic potential of probiotics to treat other major health problems, such as obesity, liver disease, fertility problems, high cholesterol and mood disorders, is also being tested. 56 Lastly, probiotics are thought to help improve cancer treatment as certain strains appear to optimize treatments (and/or reduce their toxicity) for colon, lung and kidney cancers, etc. 60,62
Focus on microRNAs, revealed by transcriptomic analysis
Discovered in the 1990s, microRNAs are of great interest to researchers as these fine regulators of gene expression are involved in many cellular processes. MicroRNA dysfunctions have been linked to a number of diseases, including cancer 63, and they are now being studied as therapeutic targets. 64 They also regulate interactions between the body's cells and the microorganisms in the microbiota.
However, probiotics seem to be able to modify their expression, for example when it is associated with intestinal inflammation. The possibility of using probiotics to act on microRNAs in order to balance the microbiota and treat certain diseases, particularly digestive diseases, looks very promising. 65
Consortia pack an even bigger probiotic punch
Probiotics are also undergoing change as scientists are experimenting with them in groups... and in pieces! The balance of the microbiota depends on the interactions between its microorganisms, and several species may be abnormally underrepresented in the event of dysbiosis. Inspired by the success of (sidenote:
Fecal transplantation
This therapeutic procedure consists in placing stool from a healthy donor in a patient’s digestive tract in order to restore the balance of their intestinal flora. For the time being, it is only approved for the treatment of recurrent Clostridioides difficile infections.
Quigley EMM, Gajula P. Recent advances in modulating the microbiome. F1000Res. 2020;9:F1000 Faculty Rev-46.) which incorporates an entire bacterial ecosystem, researchers are currently testing consortia of probiotics, i.e., formulations of several strains acting as a 'network' and in synergy 56 to achieve a defined therapeutic effect. 66
Have you ever heard of postbiotics?
Post bio...what? Postbiotics! 67 These are not whole, live microorganisms, as probiotics must be, but microbial fragments, inactivated strains (the cell is dead and no longer multiplying) or bacterial metabolites (proteins, enzymes, etc.) capable of providing benefits to the host. They are beneficial because they are easy to produce and preserve, and they are said to have similar or even superior effects to their probiotic counterparts. 56,68 Further studies are needed to confirm these encouraging initial results.
Bacteriophages: viruses that can kill bacteria....
But that's not all... Research into phage therapy, i.e. viruses that specifically attack certain pathogenic bacteria in the microbiota, is being resumed after decades of dormancy. Recent research suggests that phages could become part of the therapeutic arsenal for fighting multidrug-resistant infections. They could also help to correct the dysbiosis associated with certain diseases or serve as a 'means of transport' for targeted drugs. Further scientific work and clinical trials are once again needed before phage therapy can become one of the new, effective and safe options for tomorrow's medicine. 69
The Biocodex Microbiota Institute is dedicated to education about human Microbiota for General Public and Healthcare Professionals, it doesn't give any medical advice.
We recommend you to consult a healthcare professional to answer your questions and demands
11 Zallot, Camille : Transplantation de microbiote fécal et pathologies digestives, La Lettre de l'Hépato-gastroentérologue, Vol. XXI -n° 1, janvier-février 2018.
Celiac disease is an autoimmune digestive disease caused by a gluten intolerance. Various factors are at work, including an imbalance in the intestinal flora.
Gluten is a substance that is naturally present in wheat, barley, and rye. Unlike a gluten allergy, intolerance appears slowly and can go unnoticed for many years. In Western countries, between 0.7 and 2% of the population is affected.
An often asymptomatic disease
In its classic form, celiac disease starts around the age of six months, after the introduction of the first cereals into the diet. The classic symptoms are chronic diarrhea, lack of appetite, and apathy. However, most often celiac disease is asymptomatic.
A genetic predisposition at fault?
Celiac disease appears in people who have a genetic predisposition to it. Their immune system produces antibodies in the presence of gluten that attack the wall of the intestine. The result is that digestion is altered and nutrients aren’t absorbed as well. Other factors are involved such as the age at which gluten was introduced and repeated intestinal infections. The gastrointestinal microbiota may also play a triggering or aggravating role, according to a hypothesis that is supported by the existence of dysbiosis in these patients. The gastrointestinal flora contains fewer beneficial bacteria and more potentially pathogenic germs in comparison to healthy subjects. A gluten-free diet reduces this imbalance, but cannot fully correct it.
Diagnosis rests on a clinical examination and the presence of indicative signs, along with the search for specific antibodies in the blood and a biopsy (if necessary). Genetic predisposition has been shown through gene study (HLA typing).
Modifying the microbiota as prevention
The only treatment for celiac disease is to remove gluten from the diet. However, another approach – targeting the dysbiosis – has researchers interested. It consists of modifying the gastrointestinal microbiota to prevent the disease from developing, in cases of increased genetic risk, or to improve forms that are severe or even resist the gluten-free diet.
Cystitis is inflammation of the bladder, most often caused by urinary infection. The bacteria Escherichia coli, coming from the intestine, are the primary cause. Women are affected much more than men.
Cystitis affects 30% of women at least once in their life, with a spike in frequency between the ages of 20 and 30. It is 50 times more common in women than men. Symptoms include a burning sensation when urinating, the pressing need to urinate, and cloudy and unpleasant-smelling urine. It is simple to treat, but reoccurs frequently.
Women the most affected
Certain factors make women more likely to be affected: the shorter length of the urethra, sexual contact, catheters, urinary incontinence, menopause, and pregnancy. Anatomical anomalies and diabetes are also risk factors. Too much or too little intimate hygiene are also implicated in the appearance of cystitis.
An intestinal origin
In 90% of cases, cystitis is caused by Escherichia coli bacteria. These bacteria are naturally present in the intestinal microbiota. They can penetrate into the urethra, travel to the bladder, and multiply there.
Standardized treatment
The normal and most effective treatment for cystitis is antibiotics. However, recurrence is common. Some measures can prevent this (drinking water, hygiene, etc.). Studies have shown the benefit of taking probiotics, such as certain lactobacilli. It should be noted that cranberry may play a role in preventing recurrence of cystitis, but the effect has not yet been clearly demonstrated.
Children, teenagers, adults... almost everyone has had gastroenteritis at least once in their life. Although the disease is the world’s second most common cause of death,1 there is no cause for concern, since infectious gastroenteritis can be avoided through hygiene measures and treatment is steadily improving.2 Moreover, restoring the gut microbiota can limit the severity and duration of symptoms.3
What is infectious gastroenteritis? What link does it have with the gut microbiota?
A diarrheal disease, gastroenteritis frequently involves severe symptoms which disappear rapidly in most cases.4 Patients display an imbalance of the gut microbiota,5 which may persist after the resolution of the infection, and which has been associated with an increased risk of developing chronic disorders.6
Did you know?
The word “gastroenteritis” comes from the Greek words gastron, meaning “stomach”, and enteron, meaning “small intestine”, in other words, an inflammation of the stomach and small intestine.7
Generally benign in Western countries, infectious gastroenteritis is a leading cause of death in the developing world, particularly among children under 5 years of age.4 It accounts for 10% of all child deaths in developing countries, where it represents a major public health concern.1 The high mortality rates in developing countries8 are often9 linked to the severe dehydration that it causes. The disease is caused by the ingestion of (sidenote:
Pathogen
A pathogen is a microorganism that causes, or may cause, disease.
Pirofski LA, Casadevall A. Q and A: What is a pathogen? A question that begs the point. BMC Biol. 2012 Jan 31;10:6.) microorganisms, most frequently viruses, in which case it is known as viral gastroenteritis.
Rotavirus is one of the main causes of viral gastroenteritis worldwide and of fatal diarrhea in children in developing countries, despite the availability of a vaccine.10 Other viruses, such as norovirus or adenovirus, may also be to blame.4 Moreover, gastroenteritis can also be caused by bacteria (bacterial gastroenteritis) or parasites, particularly during travel.7 However, the pathogen involved is rarely identified.11
Contamination occurs via contaminated food or water, or directly through physical contact aggravated by poor hygiene.6 Although data on the association between the gut microbiota and gastroenteritis are still very limited, patients display a gut imbalance ( (sidenote:
Dysbiosis
Generally defined as an alteration in the composition and function of the microbiota caused by a combination of environmental and individual-specific factors.
Levy M, Kolodziejczyk AA, Thaiss CA, et al. Dysbiosis and the immune system. Nat Rev Immunol. 2017;17(4):219-232.)) during infection, regardless of the cause.5,12,13 Studies show that children with severe or complicated viral gastroenteritis, and particularly those infected with rotavirus, display a lower gut microbiota diversity than healthy children.14 Lastly, other studies suggest that changes in the gut microbiota may persist over the long term and could have adverse effects on health, such as contributing to the development of irritable bowel syndrome.15 However, current data on the gut microbiota’s contribution to the development, complications and outcome of the disease require further investigation.
Symptoms at times severe but not long-lasting
In addition to diarrhea (defined as three or more loose or watery stools in one day)6, symptoms may include nausea, vomiting, abdominal cramps, fever or anorexia.16 Symptoms of viral gastroenteritis typically last less than a week and usually improve within 1-3 days.4 Special attention should be paid to children, the elderly and immunocompromised individuals, who are at greater risk of dehydration.4 In some cases, the doctor may order additional tests (stool analysis, blood tests, etc.) to rule out other conditions.4
Antibiotics often ineffective or even counterproductive
Regardless of the cause of infectious gastroenteritis, the treatment is symptomatic.4 For diarrhea, rehydration is the main treatment.6 Antibiotic treatment is not essential and is only justified where a bacterial cause has been established for the diarrhea.11 With viral gastroenteritis, antibiotics may even be counterproductive.11 On the other hand, probiotics, which aim to restore the gut microbiota, may limit the severity and duration of symptoms.7,17
This article is based on scientifically approved sources but is not a substitute for medical advice. If you or your child display symptoms, please consult your family doctor or pediatrician.