As Gram-negative infections rise, broad-spectrum antibiotics act like a wildfire, destroying both harmful and beneficial bacteria. Lolamicin, a new antibiotic, targets only the harmful bacteria, sparing the gut microbiota and offering precise, safer infection treatment.
As (sidenote:
Gram-negative bacteria
A group of bacteria characterized by their unique cell wall structure, which makes them resistant to many antibiotics and often more challenging to treat.
) bacterial infections rise, our gut microbiome—home to trillions of beneficial bacteria—is under siege from broad-spectrum antibiotics. These drugs, though effective against infections, often wipe out our gut’s beneficial bacteria, leading to secondary infections. It's like using a sledgehammer to crack a nut. There’s an urgent need for antibiotics that zero in on the bad guys without harming the good ones.
This is where lolamicin comes in. Researchers have been working to design an antibiotic that specifically targets Gram-negative bacteria 1.
The secret weapon? The Lol lipoprotein transport system, a critical mechanism exclusive to these harmful bacteria. By disrupting this system, lolamicin can take out the pathogens while leaving our beneficial bacteria unscathed.
What are Gram-negative bacteria?
Gram-negative bacteria have a unique cell wall structure that makes them resistant to many antibiotics.
Importance in the microbiome:
47% of the gut microbiome consists of Gram-negative bacteria.
They play crucial roles in digestion and immunity.
Precision medicine: the art of crafting lolamicin
Developing (sidenote:
Lolamicin
A newly developed Gram-negative-selective antibiotic that targets the Lol lipoprotein transport system, effectively killing pathogenic bacteria without disrupting the gut microbiome.
) was no small feat. Imagine trying to craft a key that perfectly fits a lock without disturbing the surrounding structure. Researchers began with whole-cell screens, identifying compounds that could inhibit the Lol system in a group of specific bacteria. Through a series of tweaks and modifications, they engineered a hybrid scaffold that led to the creation of lolamicin.
Understanding Antibiotics
Antibiotics are drugs used to treat bacterial infections.
inhibit protein synthesis: Prevents bacteria from producing essential proteins (e.g., tetracyclines)
block DNA replication: Stops bacterial growth by interfering with DNA processes (e.g., quinolones)
This new antibiotic was put through rigorous tests and delivered impressive results. Lolamicin showed potent activity against over 130 different strains of (sidenote:
Multidrug-resistant
Describes bacteria that have developed resistance to multiple classes of antibiotics, making infections caused by these bacteria particularly difficult to treat.
), including notorious troublemakers like E. coli and Klebsiellapneumoniae. In mouse models of severe infections, lolamicin significantly reduced bacterial loads and improved survival rates, outperforming existing antibiotics.
Antibiotic Awareness
WAAW! Warning:
"Antibiotics are not automatic" – Use antibiotics responsibly to prevent resistance.
Overuse and misuse of antibiotics can lead to resistant bacterial strains, making infections harder to treat.
Always consult a healthcare professional before taking antibiotics.
Targeting the villains, sparing the heroes
But the real game-changer is lolamicin’s ability to preserve the gut microbiome. Unlike broad-spectrum antibiotics that ravage the gut's bacterial community, lolamicin treatment resulted in minimal changes. This was confirmed through advanced DNA sequencing techniques, which showed that the diversity and richness of the gut microbiome were maintained. Remarkably, lolamicin-treated mice could fend off secondary infections from Clostridioidesdifficile, a common complication of antibiotic use.
1 in 3
people had been informed by their healthcare professionals that taking antibiotics could have negative consequences on the balance of their microbiota
Although further validation in human trials is needed, lolamicin represents a revolutionary step forward. It's not just about fighting infections—it's about doing so with precision, ensuring our beneficial bacteria remain unharmed. This advancement heralds a new era in medicine, where antibiotics are tailored to target pathogens precisely, safeguarding our overall health.
Despite its strange-sounding name, functional dyspepsia is a common digestive disorder. Characteristic symptoms include stomach pain or heartburn, the feeling of an overfull stomach, discomfort, and nausea. Although not life-threatening, quality of life is affected by this disorder, in which the gut microbiota appears to be involved. Symptoms can be relieved by changing our diet or, potentially, by modifying the gut flora using probiotics.
Little known to the general public, functional dyspepsia (FD) is a very common gastrointestinal disorder that is under-diagnosed and still poorly understood today. FD accounts for 3% to 5% of GP visits in North America 1 !
The term dyspepsia comes from the Greek “dys” (poor) + “pepsis” (digestion).
Functional dyspepsia’s varied symptoms are always associated with a feeling of poor digestion 2:
feeling full long before you’ve finished your meal
the feeling of having eaten too much (stomach feels heavy and bloated), despite having eaten a perfectly reasonable-sized meal
pain or burning in the upper stomach
loss of appetite
belching or hiccups
nausea or even vomiting
Warning!
Symptoms must be long-lasting to qualify as functional dyspepsia: they must have been experienced for at least six months and present for at least three consecutive months.
postprandial distress syndrome, characterized by the feeling of a bloated stomach (postprandial fullness) after a meal or by feeling full before the meal is over
epigastric pain syndrome (concerning the upper and mid-abdomen area), where symptoms are not directly related to the meal (heartburn, etc.)
Did you know?
The disorder is called functional dyspepsia since it is not accompanied by any structural abnormality in the digestive organs and tissues. Symptoms cannot be explained by the presence of a lesion in the stomach (no ulcers) or any other organic or structural abnormality: all tests (gastroenteroscopy, ultrasound, CT scan, etc.) come out negative.
How common is the disease? Who is most at risk?
Studies suggest that 10% to 30% of adults and 3% to 27% of children worldwide are affected by functional dyspepsia 2. Women, smokers, and users of non-steroidal anti-inflammatory drugs (ibuprofen, ketoprofen) are at greater risk 3.
7%
of adults are affected by functional dyspepsia ⁴
3% to 27%
of children in the world are affected by functional dyspepsia ⁴
The consequences for patients are far from negligible: two-thirds of those affected by functional dyspepsia suffer from persistent and irregular symptoms that can affect their quality of life and well-being 1.
What factors are associated with functional dyspepsia?
Lifestyle, diet...
Diet
Increasingly clear is the role played by diet in triggering functional dyspepsia symptoms. The culprits? Above all, fatty foods. But they’re not alone. Carbohydrate-containing foods, milk and dairy products, citrus fruits, spicy foods, coffee, and alcohol, have also been implicated 5. However, the results of these studies remain uncertain.
Which foods are associated with which symptoms?
Feeling too full after a meal: red meat, bananas, bread, wheat, cakes, pasta, sausages, fried foods, beans, mayonnaise, milk, chocolate, eggs, sweets, oranges and other citrus fruits
Belching: soft drinks, onions, beans, milk, and bananas
Burning in the upper stomach: coffee, cheese, onions, pepper, milk, chocolate, pineapple 5
The mind may also play a role, with the memory of a bad experience leading patients to anticipate symptoms and over-experience them when exposed again. Experience has shown that distracting a patient with a cognitive task is enough to make them forget about their symptoms. Conversely, stating that the fat content of a yogurt is higher than it actually is increases the nausea felt by patients
FODMAPs and dyspepsia
FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are carbohydrates that humans have trouble digesting. They are thus fermented by gut bacteria (particularly Bifidobacteria), resulting in the production of gas and, therefore, bloating. Other potential effects include increased water volume in the digestive contents and excessive production of (sidenote:
Short chain fatty acids (SCFA)
Short chain fatty acids (SCFA) are a source of energy (fuel) for an individual’s cells. They interact with the immune system and are involved in communication between the intestine and the brain.
Silva YP, Bernardi A, Frozza RL. The Role of Short-Chain Fatty Acids From Gut Microbiota in Gut-Brain Communication. Front Endocrinol (Lausanne). 2020;11:25.) (propionate, butyrate, and acetate). Recent clinical trials suggest FODMAPs may be involved in the pathogenesis of functional dyspepsia 6.
Stress and anxiety
functional dyspepsia patients are often stressed and anxious: one large study showed thatanxiety was clearly linked to the disease, and more specifically to postprandial distress; another study of 18,000 Japanese showed that patients with functional dyspepsia symptoms felt more stressed on a daily basis, more often mentioned not getting enough sleep, and complained more of difficulties in falling asleep 5.
Functional dyspepsia patients generally report lower levels of physical activity. This is unfortunate since it appears that sport can actually reduce symptoms, and improve transit and gas evacuation in people suffering from bloating 5.
A study of 2,560 Swedes shows that smokers are at greater risk of postprandial distress syndrome: smoking 10 to 19 cigarettes a day increases the risk by 42%, while smoking more than a pack a day more than doubles the risk 7.
Obesity
Obesity is associated with many gastrointestinal symptoms, including functional dyspepsia. Several hypotheses have been put forward: for example, in obese people, the oral and gut receptors responsible for alerting the body to the presence of fats may be altered, amplifying the gastrointestinal effects in these patients, making them more sensitive to dietary fats 5.
Some specialists also point to a reciprocal link between functional dyspepsia and (sidenote:
Metabolic syndrome
Metabolic syndrome, also known as syndrome X, is characterized by the accumulation of several metabolic disorders in the same individual, including a large waist circumference (due to excess abdominal adipose tissue), hypertension, abnormal fasting blood sugar levels or insulin resistance, and dyslipidemia.
), with each promoting the other, creating a vicious circle 1.
Helicobacter pylori bacteria
Since the 1980s, it has been known that the stomach, although highly acidic, is not sterile. It even harbors a community of microorganisms, including the bacterium H. pylori. However,infection by H. pylori appears to lead to the onset and progression of functional dyspepsia: patients with a history of H. pylori infection have a higher risk of developing functional dyspepsia 2.
What role does the microbiota play?
Dysbiosis, the role of metabolites...
Dysbiosis throughout the digestive system
The digestive tract is home to almost 100 billion microorganisms from over 1,000 different species, which together are known as the gastrointestinal microbiota.
Proteobacteria, Firmicutes, Actinobacteria, and Bacteroidetes dominate this community, making up more than 98% of the gut microbiota, with Firmicutes predominating, followed by Actinobacteria and Bacteroidetes2. At least in healthy patients. In those suffering from illnesses such as functional dyspepsia, this balance is not found; instead, dysbiosis is observed throughout the digestive system, from mouth to anus2.
In functional dyspepsia patients, studies have found, for example:
a higher abundance of Firmicutes, streptococcus (associated with symptoms in the upper stomach), Bifidobacterium and Clostridium
a lower abundance of Prevotella (accompanied by more symptoms of discomfort after eating)
The microbiota’s role in functional dyspepsia is far from limited to the bacteria present, since each of these bacteria secretes various active molecules, both beneficial and harmful, that are closely linked to host health and to the onset and progression of numerous diseases 2,3. For example:
while others are harmful to the host (e.g. pro-inflammatory sphingolipids produced by Bacteroidetes and Prevotellacae) 3
What mechanisms are involved?
Immunity, the gut-brain axis...
While many gray areas remain, researchers believe that the mechanisms behind functional dyspepsia are likely to be multifactorial and vary from patient to patient8. Thus, a range of mechanisms are involved in functional dyspepsia:
Disruption of the gut barrier
In normal circumstances, food passing through our digestive system remains isolated from our body by a barrier, the intestinal mucosa. This barrier is semi-permeable: it allows nutrients to be absorbed but bars passage to the various harmful substances and pathogens ingested along with our meal 2.
In functional dyspepsia patients, the integrity of this mucosa is compromised, so much so that it performs its filtering role less effectively
Disruption of gut immunity
In functional dyspepsia patients, there appears to be an excessive immune response: 40% of patients present inflammatory cells infiltrated into the duodenum, while a proliferation of bacteria (particularly oral bacteria) 9 is frequently observed in the small intestine, which may activate this immune response. Indeed, some researchers believe that a greater focus on the microbiota of the (sidenote:
Small intestine
Section of the digestive system between the stomach and the large intestine (i.e. the colon) essential for the digestion and absorption of nutrients. Measuring 21 to 23 feet, it is the longest portion of the digestive tract, comprising the duodenum, then the jejunum, and finally the ileum.
) is required in order to better understand the pathogenesis of functional dyspepsia 9.
Is a proliferation of bacteria in the small intestine to blame?
A proliferation of bacteria in the small intestine (orsmall intestinal bacterial overgrowth – SIBO) may play a role in the pathogenesis of functional dyspepsia; indeed, this overgrowth appears to be more frequent in patients with functional dyspepsia than in those who do not suffer from the disorder 10,11. Among functional dyspepsia patients, those prescribed PPIs (proton pump inhibitors, drugs used to reduce gastric acid secretion) appear to be at greater risk of SIBO12. By reducing stomach acidity, PPIs diminish the chemical barrier which is supposed to destroy a range of pathogenic micro-organisms using hydrochloric acid secreted by the stomach walls. This may explain the presence of excess bacteria in the small intestine, which lies just below the stomach.
However, evidence of a link between functional dyspepsia and SIBO remains tenuous: in the absence of easy access to duodenal flora, studies generally rely on the detection of gases in patients’ exhaled breath. This test is easy to perform and non-invasive but clearly lacks reliability 11.
Deregulation of the gut-brain axis
There are complex interactions between the gut microbiota, the digestive system, and the central nervous system. This microbiota-gut-brain axis explains why stress can cause stomach ache, or why changes in the gut flora can alter intestinal motility and “inform” the brain, which in turn can regulate the gut. However, functional dyspepsia has been shown to be closely linked to gastrointestinal motility disorders (which are under cerebral control) and to gastrointestinal hypersensitivity, all of which are linked to the gastrointestinal microbiota 2. From here to suggesting that everything is linked is only a short step...
The presence of nutrients in the interior of the digestive tract produces signals that alter digestion. For example, a high-fat meal emains in the stomach longer, since gastric emptying is delayed. In functional dyspepsia patients, food ingestion may be associated with exaggerated signals from the gastrointestinal tract. This results in a whole series of symptoms which bear no relation to reality, such as feeling full when a meal has only just begun, hypersensitivity to gastric distension, and so on. 5
What are the existing and potential treatments for functional dyspepsia?
Diet, probiotics...
Diet
Logically, since diet is thought to play a role in functional dyspepsia, adapting it may improve symptoms. However, there is a dearth of studies highlighting the effects of specific diets. Nevertheless, experts believe that a large proportion of patients would benefit from a lower-fat diet and smaller meals eaten more often. In fact, functional dyspepsia patients are already doing so in practice: they have a slightly reduced dietary fat intake and tend to eat smaller meals more frequently 5.
Other patients would benefit more from avoiding spicy or acidic foods (tomatoes, citrus fruits, etc.) or foods rich in fiber or FODMAPs, which cause bloating. However, these restrictions should be managed with care so as to avoid an unbalanced diet 2.
Proton pump inhibitors (PPIs) are drugs used to reduce gastric acid secretion. They are prescribed by doctors to treat gastroesophageal reflux disease (GERD) and peptic ulcers.
In the short term, proton pump inhibitors (PPIs) may improve functional dyspepsia symptoms. However, their long-term use seems to go hand in hand with an increase in Streptococcus and, thus, a harmful dysbiosis 13.
Antibiotics to eradicate H. pylori
According to the American College of Gastroenterology and the Canadian Association of Gastroenterology, functional dyspepsia patients under 60 years of age should first be screened for H. pylori. If the test proves positive, antibiotics should be prescribed to eradicate the bacteria.
However, this strategy has its limits: only 1 in 10 patients will experience an improvement in their symptoms, while the remainder will see their symptoms worsen 14.
Since dysbiosis of the gastrointestinal microbiota is closely linked to the onset and progression of functional dyspepsia, regulating the gastrointestinal microbiota has logically been put forward as a potential treatment 2. The role of probiotics may be multifactorial15 :
restoration of commensal flora eliminated by pathogens
restoration of gut barrier permeability
reduction of visceral hypersensitivity
local and systemic anti-inflammatory action
regulation of intestinal motility
All these benefits are thought to reduce symptoms of functional dyspepsia 15.
A large number of clinical studies seem to confirm “in practice” that probiotics can improve patients’ symptoms 2,15 .
However, the results published over the last 15 years are not sufficient to draw conclusions, since they have a number of shortcomings: the definition of the disease has continued to evolve; studies often confuse functional dyspepsia (long-lasting) with H. pylori infection (short-term); the probiotics used vary widely from one study to another; reports of symptoms remain unreliable due to a lack of clinical objectivity, and so on 15. Further research is still needed.
Alternative therapies
Various alternative therapies have been recognized as safe and effective treatments for functional dyspepsia:
cognitive behavioral therapy, commonly used to treat stress and anxiety, helps the patient identify the thoughts or behaviors that lead to or exacerbate the expression of symptoms
hypnotherapy, where the patient, in a state of hypnosis, is more receptive to therapeutic suggestions
The potential of virtual reality is also being explored 14.
Prebiotics, probiotics, postbiotics... Behind these confusing terms actually lies an exciting universe related to our health. These "biotics" are the discreet little hands working behind the scenes to take care of our precious intestinal microbiota. Ready to lift the veil on their unique roles and fundamental differences? In this article, we will unravel the threads of this microscopic web to allow you to tame these unsuspected allies of well-being. Let's explore together this fascinating ecosystem that resides in each of us!
We're about to dive into the fascinating world of "biotics." Now, you might be thinking, "What in the world are 'biotics'?" Well, it all goes back to an ancient Greek word, "bíos," which simply means "life." From that root word, we get terms like probiotics, prebiotics, postbiotics, synbiotics. These aren't just fancy scientific names – they're like the different parts that make up a lively neighborhood, each playing a unique role in keeping things running smoothly.
Imagine you're the new resident on the block, and a friendly neighbor offers to show you around, pointing out all the key people and places that make the community tick. That's what we're doing here – getting a local's tour of the "biotics" neighborhood inside your body.
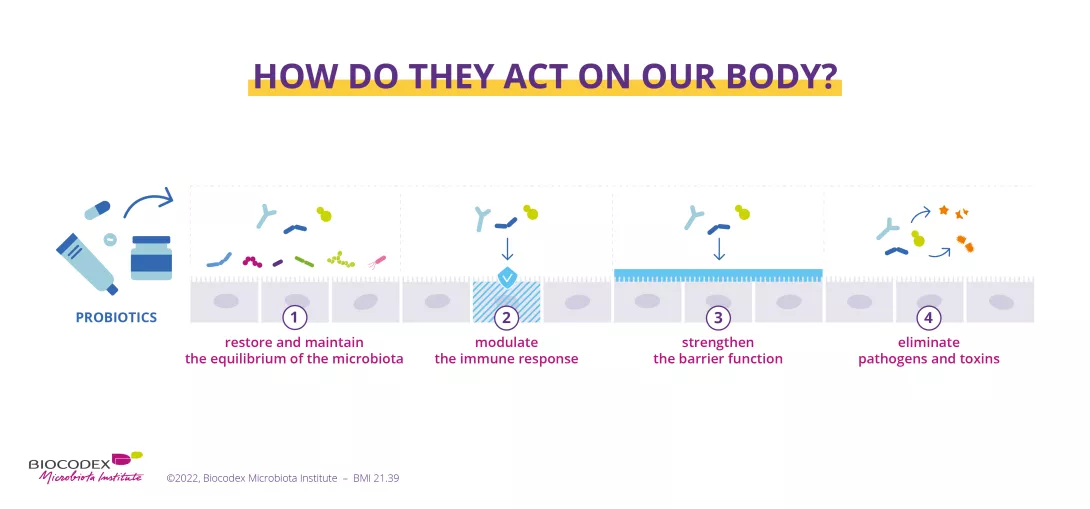
Probiotics: your body's helpers
In our city of health, probiotics are like our visiting beneficial friends – live microorganisms that take up residence within us and contribute to our well-being. As defined by the World Health Organization (WHO) and the International Scientific Association for Probiotics and Prebiotics (ISAPP), probiotics are "live microorganisms which, when administered in adequate amounts, confer a health benefit on the host."1
In simpler terms, they are beneficial microbes such as bacteria, yeast, … that support our overall well-being. Probiotics contribute to our health in various ways, such as:
promoting a balanced microbiome 2
inhibiting the growth of pathogens inside the human body 3
improvement in barrier and metabolic functions of targeted organs 4, 5, 6
One widespread misconception is that all fermented foods, such as yogurt, kefir, or kombucha, are inherently probiotic.9 While fermentation can introduce beneficial bacteria, not all fermented products contain live, probiotic strains that meet the criteria set forth by health authorities. 10 However, some fermented foods are fermented using a microbe proven to be a probiotic, or have been supplemented with probiotics in sufficient quantities to offer health benefits.
It's essential to carefully read labels and rely on reputable sources to ensure you're consuming products with scientifically and clinically validated probiotic cultures. Additionally, some assume that probiotics are a one-size-fits-all solution, but different strains can have varying effects on different individuals and health conditions.1, 11 Consulting with healthcare professionals and following evidence-based guidelines is crucial for optimizing the benefits of probiotics based on your unique needs and circumstances.
Image
If you want to learn more about probiotics, you can read our dedicated section here:
Prebiotics: food for the good guys – but not only!
Prebiotics are defined as "a substrate that is selectively utilized by host microorganisms conferring a health benefit." 12, 13 Unlike probiotics, prebiotics themselves are not live microbes but rather serve as fuel for the existing beneficial bacteria in our microbiome. It's a common oversimplification to describe prebiotics as "food for probiotics."
While prebiotics do support probiotic growth, their beneficial effects stem from the activity of the resident gut microbiota, which metabolize these compounds, indirectly conferring physiological advantages to the host – us! Moreover, not all dietary fibers are prebiotics, and not all prebiotics are fibers.14 This distinction is often overlooked, leading to misconceptions about their definitions and functions.
Imagine prebiotics as favorite restaurants for your helpful bacteria. Foods like bananas, onions, and garlic are rich in substances such as inulin and galacto-oligosaccharides (GOS) that act as prebiotics. When your beneficial bacteria dine on these foods, they can increase the production of molecules, i.e. metabolites, such as short-chain fatty acids (sidenote:
Short chain fatty acids (SCFA)
Short chain fatty acids (SCFA) are a source of energy (fuel) for an individual’s cells. They interact with the immune system and are involved in communication between the intestine and the brain.
Silva YP, Bernardi A, Frozza RL. The Role of Short-Chain Fatty Acids From Gut Microbiota in Gut-Brain Communication. Front Endocrinol (Lausanne). 2020;11:25.) acetate, propionate, and butyrate which in turn can improve your health. 15
Beyond supporting gut health, prebiotics have been linked to re-balancing the microbiota for better defense against pathogens, 16weight management, 17 better mineral absorption, 18 etc. Their benefits extend beyond just the gut. 19
We have also prepared a dedicated section about prebiotics and their health benefits here:
After probiotics have completed their visit of the city, they leave behind gifts known as postbiotics. These are like the products and services that businesses in a city provide after taking in raw materials. Postbiotics include beneficial substances like vitamins and (sidenote:
Short chain fatty acids (SCFA)
Short chain fatty acids (SCFA) are a source of energy (fuel) for an individual’s cells. They interact with the immune system and are involved in communication between the intestine and the brain.
Silva YP, Bernardi A, Frozza RL. The Role of Short-Chain Fatty Acids From Gut Microbiota in Gut-Brain Communication. Front Endocrinol (Lausanne). 2020;11:25.). They're the rewards your body gets from the probiotics' hard work.
This definition was revised many times, and the Scientific Community have now reached a consensus: “postbiotic is a preparation of inanimate microorganisms and/or their components that confers a health benefit on the host.” This means that postbiotics are not just the “re-purposed” waste of the probiotics (or their end-products), but they are also the “dead” probiotics themselves and fragment components!20
Such as probiotics, postbiotics have been shown to strengthen the barrier function, reduce inflammation, and exhibit antimicrobial activity against pathogens, thereby promoting overall health. 21Their beneficial properties also extend beyond the gut with benefits for skin and vaginal health and potentially addressing skin and vaginal conditions.22, 23
You may have heard additional names such as Parabiotics, Paraprobiotic or Proteobiotics. Indeed, some researchers have tried to define further the different elements or body parts of the postbiotic component, meaning dead cells, components of the cells and the metabolites produced by those microbial cells.
While Parabiotics and Paraprobiotic are synonymous, they’re used to describe the inactivated microbial cells, either intact or broken; think of them as the "ghosts" of those helpful microbes still being able to lend a hand. 24
On the other hand, Proteobiotics are natural metabolites produced by the probiotic during fermentation. 25, 26
However, there is no consensus agreement on these possible definitions, and they all fall under the ISAPP definition of Postbiotic. 20
Synbiotics in action and psychobiotics curious case
Synbiotics are like community projects that bring everyone together for a common goal. 27 They combine probiotics and prebiotics in a single product, ensuring that the good bacteria not only have a place to live but also plenty of their favorite food right from the start. This combination can be found in some yogurts and dietary supplements, designed to work together to provide an even greater health benefit.
On the other hand, Psychobiotics are a whole new category of probiotics and prebiotics that can actually benefit your mental health when consumed properly.28They work through something called the gut-brain axis. Basically, your gut and brain are physically connected and are in constant communication. The microbes living in your intestines can send signals to your brain that impact your mood, cognition, and even behaviors.
Researchers are really excited about the potential of psychobiotics. Early studies show they may help prevent or improve conditions like neurodegenerative diseases like Alzheimer's or Parkinson's. Some evidence even suggests psychobiotics could play a therapeutic role in treating psychiatric disorders like depression or anxiety. 29
You can find out more about the interaction between the gut and the brain here:
Finally, it's essential to differentiate antibiotics from the other "biotics." While antibiotics are crucial life-saving medications for treating bacterial infections, their indiscriminate or excessive use can severely disrupt the delicate balance of the microbiome, potentially causing unintended and far-reaching consequences. 30, 31These powerful drugs don't discriminate between harmful and beneficial bacteria, which means they can decimate the vital microbial populations that promote health and immunity.
Antibiotic resistance
Furthermore, the overuse of antibiotics contributes to the alarming rise of antibiotic-resistant superbugs, posing a significant global health threat. 30 Therefore, it's imperative to use antibiotics judiciously and only when absolutely necessary, under the guidance of healthcare professionals.
Maintaining a healthy, diverse microbiome through probiotics, prebiotics, and other "biotics" can help counteract some of the collateral damage caused by antibiotics and support overall well-being.
You can find here a dedicated section about the effects of antibiotics on the microbiota and on your health:
Each year, since 2015, the WHO organizes the World AMR Awareness Week (WAAW), which aims to increase awareness of global antimicrobial resistance.
Antimicrobial resistance occurs when bacteria, viruses, parasites and fungi change over time and no longer respond to medicines. As a result of drug resistance, antibiotics and other antimicrobial medicines become ineffective and infections become increasingly difficult or impossible to treat, increasing the risk of disease spread, severe illness and death.
Held on 18-24 November, this campaign encourages the general public, healthcare professionals and decision-makers to use antibiotics, antivirals, antifungals and antiparasitics carefully, to prevent the further emergence of antimicrobial resistance.
Diarrhea kills around 1.5 million people every year.55 It is the third cause of death in children under 5.1
Most cases of acute diarrhea are due to infectious pathogens, i.e. viruses, bacteria, parasites. Rotavirus and Escherichia coli are the two most common etiological agents of moderate-to-severe diarrhea in low-income countries.1
The complex interplay between infectious agents and the microbiota
Whatever the etiological agent of infectious diarrhea, the outcome depends on complex interplays between the pathogen and the gut microbiota.
The composition of the gut microbiota can shape the outcome of an infection by a diarrheal pathogen, and be either a protective or a facilitating factor. In turn, the diversity and composition of gut microbiota can be severely altered by infectious diarrhea and a return to a "healthy microbiota" may require several weeks after diarrhea has resolved.14
A significant proportion of preventable cases
A significant proportion of diarrheal disease can be prevented through safe drinkingwater and adequate sanitation and hygiene.1
Rotavirus vaccination is another important preventive strategy, which the WHO recommends be included in all national immunization programmes and considered as a priority.56
Patient monitoring and management
The majority of infectious diarrheas are self-limiting in immunocompetent individuals. Nevertheless, some patients (with severe dehydration, more severe illness, persistent fever, bloody stools, immunosuppression…) require specific diagnostic investigation.11
The most important complication of infectious diarrhea is dehydration, which may require oral or intravenous fluid replacement therapy, depending on the degree of dehydration.1
Gut microbiota targeting strategies, essential in diarrhea prevention and management
Both the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) and the World Gastroenterology Organization (WGO) consider that some probiotic strains can be recommended by HCP:
for the prevention of antibiotic-associated diarrhea;
for the treatment of acute (viral) diarrhea in children, as they may shorten diarrhea duration.
Promising research paths involving microbiota
Future research should expand microbiome knowledge in the context of infectious diarrheas, in order to improve their prevention and management.
The optimization of microbiota profile in order to shape infectious outcomes5 and improve rotavirus vaccine efficacy29 represents a promising research path.
Not all individuals respond to intestinal infections of parasites in the same way: while some develop no symptoms at all, others experience more or less severe diarrhea, which can lead to death. The gut microbiota is increasingly cited as a key factor in explaining this variability
Intestinal parasites can be broadly classified into protozoa (single cell organisms) and helminths (multicellular, known as worms).39 Globally, there are an estimated 895 million people infected with soil transmitted helminths (STH). Intestinal protozoa (IP) have a lower overall prevalence rate, but still, over 350 million people are believed to be infected with 3 of the most common protozoan parasites40. Protozoan infections are common in low and middle income countries (LMICs). Food-chain globalisation, international travel and migration are leading to an increase in protozoan infections in high income countries, where they are more common than intestinal helminth infections.39
Giardiasis, the most common parasitic diarrhea worldwide, affects 280 million people each year.41
DIARRHEAS CAUSED BY PROTOZOAN PARASITES
The most common intestinal protozoan parasites are Giardia intestinalis (Giardia duodenalis or Giardia lamblia), Entamoeba histolytica, Cyclospora cayetanensis, and Cryptosporidium spp. Diarrheal diseases caused by these pathogens are known respectively as giardiasis, amebiasis, cyclosporiasis and cryptosporidiosis.41
Giardia intestinalis
Giardia intestinalis infects the upper small intestine altering its barrier and permeability. Between 6 and 15 days after infection, it can cause acute, watery diarrhea associated with abdominal cramps, bloating, nausea and vomiting. Giardiasis, the most common parasitic diarrhea worldwide, affects 280 million people annually. 41
Entamoeba histolytica
Entamoeba histolytica infections are usually asymptomatic but can produce an invasive disease of the large bowel (notably in immunocompromised patients) and amebic dysentery can develop. The acute phase lasts 3 weeks, with abdominal pain, bloody diarrhea and mucus in the stools. Accounting for over 26 000 deaths annually,2 amebiasis is the third leading cause of death from parasitic infections worldwide; it particularly affects people in LMICs.41
Cyclospora cayetanensis
Cyclospora cayetanensis is the only species of the genus Cyclospora that can infect humans. After an incubation period which may vary from 2 to 12 days, it typically manifests as voluminous watery acute diarrhea, abdominal cramps, nausea, low grade fever, fatigue and weight loss.41
Cryptosporidium spp.
Cryptosporidium spp. infection symptoms appear after one or two weeks of incubation: the most common clinical symptoms are acute watery diarrhea, abdominal cramps, malabsorption, nausea, vomiting and fever, lasting for approximately 5 to 10 days.41 An estimated 64 million cases of cryptosporidiosis are reported each year.40
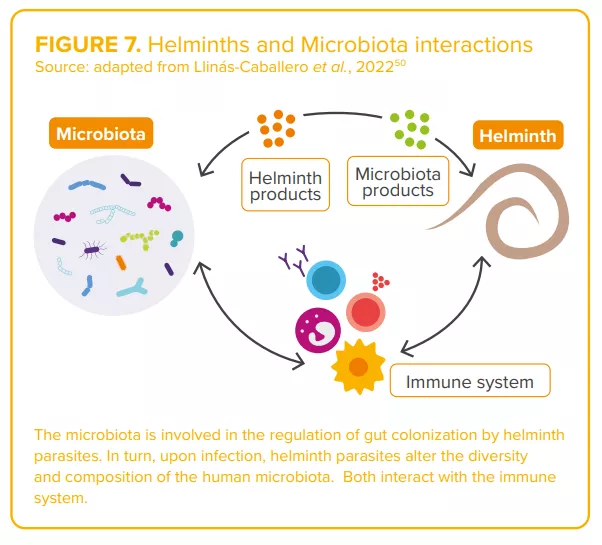
Helminth parasites and the microbiota have coexisted within their hosts, for millions of years. 50
TRAVELERS’ DIARRHEA: PARASITIC INFECTION IS COMMONLY ASSOCIATED WITH PI-IBS
While the majority of travelers’ diarrhea cases are acute and resolve spontaneously, a subset of individuals will experience persistent gastrointestinal (GI) symptoms potentially extending for weeks, months, or even years, after the initial cause has been effectively treated.52 A recent publication suggests that nearly 10% of patients experiencing travelers’ diarrhea develop persistent symptoms consistent with post-infectious irritable bowel syndrome (PIIBS). Parasitic infection, particularly giardiasis, is commonly associated with PI-IBS.53
DIARRHEAS CAUSED BY SOIL-TRANSMITTED HELMINTHS
Globally, the principal soil-transmitted helminths are the roundworm (Ascaris lumbricoides), the whipworm (Trichuris trichiura) and hookworms (Necator americanus and Ancylostoma duodenale). Symptoms experienced following helminth infection are related to the number of worms harboured: people with infections of light intensity (few worms) do not usually experience discomfort, whereas heavier infections can cause a range of symptoms including some that manifest in the intestine (diarrhea and abdominal pain), malnutrition, general malaise and weakness, and impaired growth and physical development. Soiltransmitted helminths contribute to the burden of diseases by impairing the nutritional status of the people they infect in a variety of ways: they feed on host tissues, cause intestinal blood loss and hamper the absorption of nutrients.42
Ascaris lumbricoides is the most common intestinal nematode that infects humans, with an estimated 807 - 1,221 million people infected each year. 43 Infection commonly occurs without symptoms. The symptomatic form is characterized by an early lung phase followed by a later intestinal phase, which is characterized by diarrhea, mild abdominal pain, anorexia, nausea and vomiting.41
An estimated 604-795 million people in the world are infected with Trichuris trichiura. People with heavy infections can experience frequent painful bowel movements that contain a mixture of mucus, water and blood.44
An estimated 576-740 million people in the world are infected with hookworms, usually without symptoms. Few people, especially those infected for the first time, experience gastrointestinal symptoms. The most common and serious effects of hookworm infection are intestinal blood loss leading to anaemia, in addition to protein loss.45
MICROBIOTA: A ROLE IN THE MARKED CLINICAL VARIABILITY OF PARASITIC DIARRHEA?
Parasitic protozoan infections are characterized by marked variability in their clinical presentation: they can be asymptomatic or cause diarrhea, abdominal pain, weight loss, etc. Recent studies have highlighted the potential contribution of the intestinal microbiota to this clinical variation: for instance, an abundance of Prevotella copri in the gut microbiota predicted diarrhea in the context of Entamoeba histolytica infection;46 low Megasphaera abundance prior to and at the time of Cryptosporidium detection was associated with parasitic diarrhea in infants in Bangladesh, suggesting that the gut microbiota may play a role in determining the severity of a Cryptosporidium infection.47 In turn, infection by protozoan parasites alters the gut microbiome.48,49
Regarding helminths, the complex interactions between worms and the microbiota (“two of humans’ old friends” 50) are currently under study50 (Figure7). Authors agree on the existence of a complex and dynamic interplay between parasite(s), the host microbiota and host immunity, capable of shaping the clinical outcomes of parasitic infections.46,48
Image
CLINICAL CASE by Pr. Stephen Allen
During her holiday in Asia, 36-year-old company executive develops non-bloody, slimy, smelly diarrhea with abdominal cramps and bloating.
In the second week of the illness, stool microscopy revealed giardiasis and she takes a 10-day course of metronidazole.
Over the course of the following year in the UK she experiences frequent episodes of similar symptoms, each lasting for a few days and forcing her to stay off work.
After other illnesses are ruled-out by further investigations and a clinical review, she is diagnosed with post-infectious, diarrheapredominant, irritable bowel syndrome (IBS-D), a condition that develops in 10% of patients following an acute episode of gastroenteritis.54
She finds that dietary changes and treatments for IBS-D have little effect and wants to know if she should send a stool sample abroad for microbiome analysis and whether a fecal transplant might help.
The role of persistent dysbiosis in postinfectious IBS due to parasitic infection and/or drugs used for treatment is poorly understood. More research is needed before this woman’s questions can be answered with any confidence.
EXPERT OPINION
Gut parasite infection is a common cause of disease worldwide, predominantly diarrhea with protozoans such as giardia, Entamoeba histolytica and Cryptosporidium, and anaemia with helminths. Equally, gut parasites occur as commensals and may even bring health benefits such as improving resistance to other enteropathogens and preventing allergic and auto-immune diseases. The challenge is to gain a better understanding of the complex interrelationships between different parasites, the intestinal mucosa, gut immune cells and the gut microbiota in order to be able to exploit the benefits while at the same time ameliorating adverse effects of intestinal parasitic infection.
PR. STEPHEN ALLEN Professor of Paediatrics, Liverpool School of Tropical Medicine (UK)
Usually presenting as watery diarrhea, viral diarrheas are caused by 5 main types of virus. Among them, rotavirus remains the leading cause of diarrhea-related mortalities in children under 5 years of age, this despite the availability of vaccines since 2006. Composition of the gut microbiota, implicated in viral infection outcomes, and rotavirus vaccine efficacy, could play a key role in strategies aimed at reducing the burden of viral diarrhea.
Rotaviruses, norovirus, sapovirus, astrovirus, and adenovirus: five virus types are currently recognized as the main causes of viral diarrhea.21
Of the 2 billion plus episodes of diarrheal disease that occur across the world each year, as estimated by the 2016 Global Burden of Disease (GBD) Study,2 almost 900 millions of the moderate-to-severe episodes were attributed to just three of these viruses: rotavirus, norovirus and adenovirus22.
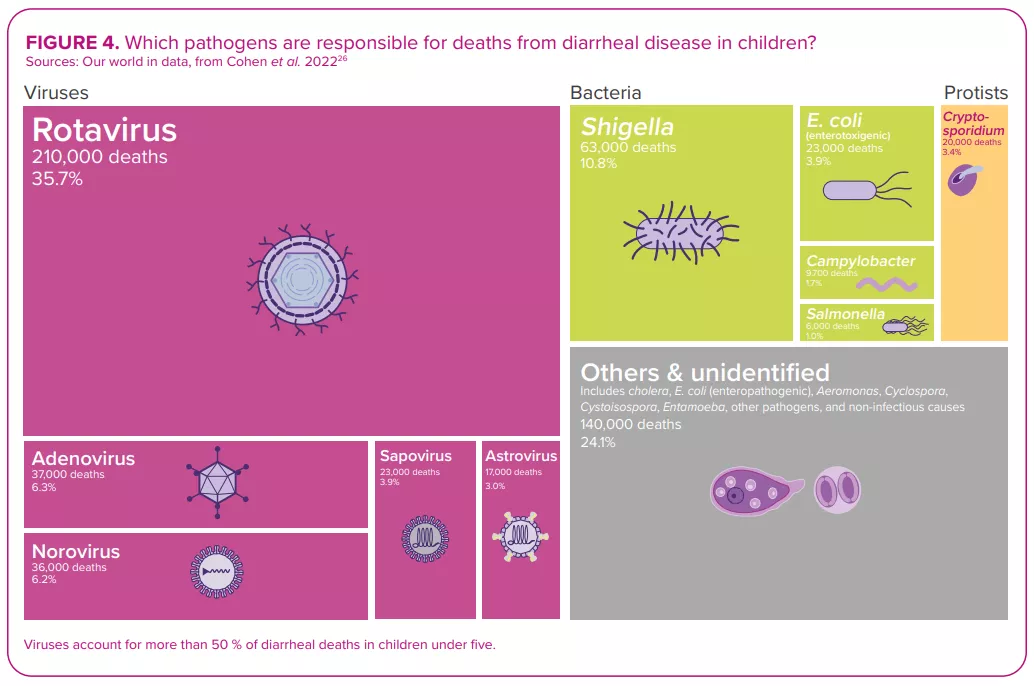
ROTAVIRUS, THE NUMBER ONE DIARRHEAL KILLER IN CHILDREN
Despite the development and availability of rotavirus vaccines since 2006,22 this virus, which causes more severe symptoms than most other enteric pathogens,22 was still responsible for over 228,000 deaths worldwide in 2016, of which over 128,000 occurred in children below the age of 52 – making rotavirus the leading cause of diarrhearelated mortalities among this segment of the population (Figure 4).
WATERY DIARRHEA
Whatever the virus that triggers an episode of diarrhea, the process of infection is broadly the same: the virus infects the epithelial cells of the small intestine and causes damage that hampers the absorption of fluid.21 Viral diarrhea usually manifests itself in the form of a watery (non-bloody) diarrhea. It can be accompanied by other symptoms, i.e. nausea, abdominal cramps, vomiting and fever,22 resulting in what is known as viral gastroenteritis.
REHYDRATION… AND PROBIOTICS
Just as for the other etiologies (bacterial or parasitic) of infectious diarrhea, management of viral diarrhea relies on oral or intravenous fluid replacement therapy, depending on the degree of dehydration.21 In addition, according to the latest conclusions of the ESPGHAN committee (2023),20 healthcare professionals may recommend some probiotic strains (L. rhamnosus, S. boulardii and L. reuteri) for the management of acute gastroenteritis in children, since there is some evidence (certainty of evidence: low; grade of recommendation: weak) of reduced duration of diarrhea, and/or length of hospitalization, and/or and stool output.
Among all diarrheal pathogens, and despite vaccine availability, rotavirus remains the number one killer of children under five years of age. 2
IMPROVING ROTAVIRUS VACCINE EFFICACY, A CHALLENGE YET TO OVERCOME
Regarding prevention, the usual preventive measures apply (ensuring safe drinking water, adequate sanitation and frequent handwashing, limiting contact with infected people, etc.). Given the considerable burden of rotavirus diarrheal disease, rotavirus vaccines are another important preventive measure.22,23
SARS-COV-2: NEW MEMBER OF THE DIARRHEAL VIRUSES CLUB
Alongside the viruses long recognized as principal causes of viral diarrhea, infection with the SARS-CoV-2, responsible for the greatest pandemic in recent times, COVID-19, may also give rise to diarrhea. In clinical studies, the incidence rate of diarrhea ranges from 2% to 50% of cases. 27 As with the respiratory tract, the angiotensin-converting enzyme 2 (ACE2) receptors are highly expressed on intestinal cells, serving as an important site of entry for the virus in the gut. The putative mechanisms leading to the development of diarrhea mainly involve angiotensin-converting enzyme 2 dysregulations following virus entry into enterocyte, which could trigger an inflammatory response, ionic imbalance and increased permeability. Furthermore, the spike protein of SARS-CoV-2 acts as an enterotoxin, with a mechanism similar to the rotavirus enterotoxin NSP4.28 Alteration of gut microbiota and side effects of medications (antiviral and antibiotics) are also thought to be involved.29
Image
Microbiota: a key role in rotavirus vaccination efficacy
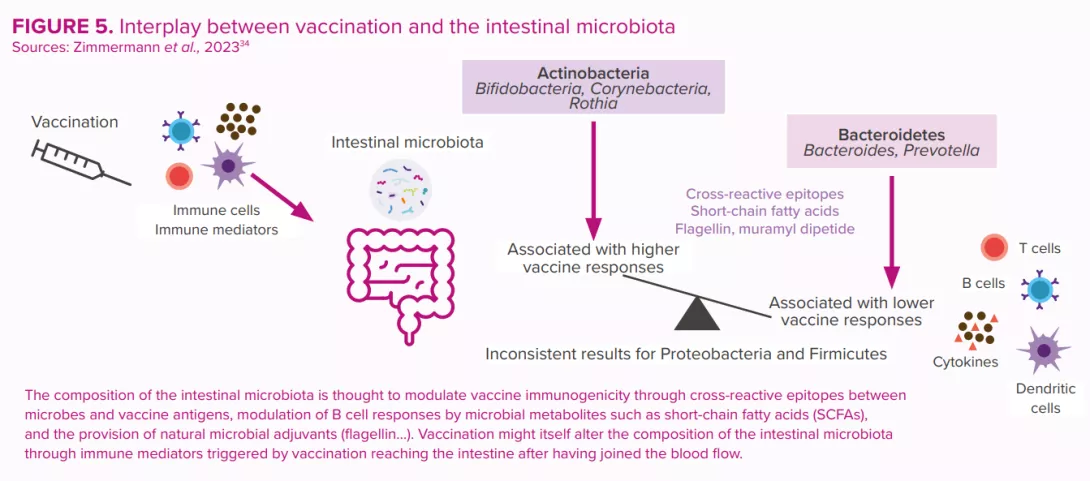
Since their introduction in 2006, oral rotavirus vaccines (ORVVs) have at a global level led to a significant drop in the number of hospitalisations and deaths due to rotavirus diarrhea.30 However, the efficacy of the vaccines has been varied, with low-income countries suffering from lower performance compared to the remarkably high efficacy (>90%) observed in higher income countries.31 Reasons for this disparity are thought to be multi-factorial (host immunity, perinatal outcomes, genetics, nutritional status, stress, tobacco and alcohol use, rural versus urban location, family size, etc.). Just as for other vaccines, the composition and function of the gut microbiota is considered to be a key factor that regulates the immune response to vaccination30,32,33 (Figure 5).
Image
These were estimated to have prevented 139,000 deaths from rotavirus among under-fives during the period 2006 to 2019, and to have prevented 15% of under-five rotavirus deaths in 2019.24 However, vaccine efficacy is region-specific and displays poor seroconversion in low-and middle-income countries. Human clinical trial data have suggested a possible link between the gut microbiota and the enteric immune system’s response to rotavirus vaccine25 (Figure 5).
Each gram of human gut content is estimated to contain at least, 108 –109 virus-like particles, the vast majority of which are phages.14
MICROBIOTA: FRIEND OR FOE IN THE ONSET OF VIRAL DIARRHEA?
In cases of viral diarrhea, as with infectious diarrhea in general, the outcome of the confrontation between pathogen and host depends on complex balances that in large part involve the microbiota.
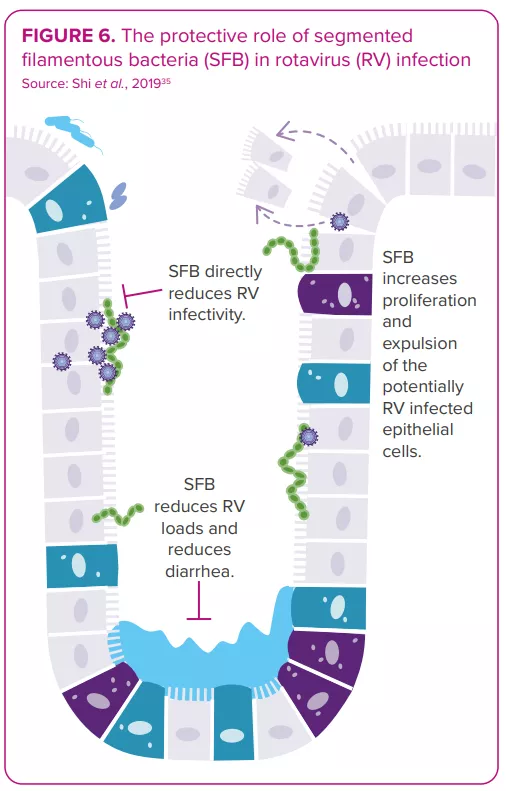
The gut microbiota displays bidirectional interactions with rotavirus and norovirus infections:14 it can either protect against or predispose the host to infection; in turn, an infection can alter the gut microbiota. Some bacteria seem able to inhibit viral infection. For example, one study shows segmented filamentous bacteria preventing and curing rotavirus infection in mouse colonies35 (Figure 6). On the other hand, in vitro and in vivo studies indicate the gut microbiota’s involvement in facilitating viral infection: certain gut microbes (e.g. Enterobacter cloacae) stimulate the ability of human norovirus to infect human B cells in vitro; microbiota elimination by antibiotics delays infection, reduces infectivity and/or viral titer of norovirus and rotavirus in mice.8,36
Therefore, any invasive pathogens might have different effects depending on the state of the gut microbiota. 3 The optimal microbiota profile and microbiota-targeting strategies that would lower the risk of infection and the following viral diarrhea remain to be characterized.37
As to the effect of viral infection on gut microbiota composition, numerous studies have documented specific patterns of dysbiosis in patients suffering from viral diarrhea compared to healthy controls25,38. A reduction of microbiota (alpha) diversity is often reported, but specific taxa increases or decreases vary widely across the studies.14 And one question remains: does the dysbiosis observed during viral diarrhea reflect a prior disposition that might have facilitated the infection, is it a state caused by the virus, or is it a combination of both?
Image
CLINICAL CASE by Dr. Marco Poeta
A 4-year-old girl presented to the paediatric emergency room with fever, diarrhea, vomiting and severe dehydration.
Since the child needed intravenous rehydration, she was admitted to the hospital.
The nasopharyngeal swab returned positive for SARS-CoV-2 infection, despite the absence of respiratory symptoms.
Stools were negative for rotavirus, norovirus, adenovirus, bacteria and parasites but positive for SARS-CoV-2.
Following the administration of probiotics, her stool frequency and consistency both recovered.
The intravenous hydration was discontinued after four days, and the child was discharged.
Diarrhea can be the only clinical manifestation of the SARS-CoV-2 infection. SARS-CoV-2 should therefore be added to the list of enteric pathogens.
The efficacy of probiotics against Covidassociated gastroenteritis observed in this clinical case has already been demonstrated via in vitro studies.
EXPERT OPINION
Probiotics are recommended as an active means of treating of viral diarrhea in children, exerting an antidiarrheal effect that restores microbiota composition from its altered state. In clinical trials, some probiotic strains reduce secretory diarrhea in a very short time, measurable within hours after the start of probiotic administration. Considering that several days are normally required to establish changes in the composition of the microbiota, the rapid efficacy of probiotics implies that there are additional positive effects. Molecules secreted by the bacteria that act directly on intestinal cells can inhibit secretory diarrhea through an antioxidant mechanism. This is defined as the "postbiotic effect". The metabolites produced by probiotics have pharmacological-like action and could represent innovative therapies for the management of viral diarrhea.
DR. MARCO POETA Paediatric Infectious Diseases Unit, University of Naples Federico II (Italy)
Antibiotics are a powerful tool in the fight against bacterial infections, however they also disrupt the protective intestinal microbiota and this can lead to unintended consequences including antibiotic-associated diarrhea (AAD) in as much as 35% of patients.17,18,19The incidence of AAD depends on several factors: 17,18,19 age (among children this percentage can reach up to 80%) 15, setting, type of antibiotic, etc. Most of the time, AAD is caused by antibiotic-induced dysbiosis, is of mild intensity and is self-limiting, lasting between 1 and 5 days.
While the etiologies for AAD are diverse, approximately one-third of AAD cases are attributed to C. difficile. Under certain conditions, C. difficile will trigger an inflammatory response leading to a range of clinical outlooks, from mild diarrhea to pseudomembranous colitis, toxic megacolon and/or death.17
ESPGHAN 2023 RECOMMENDATIONS
In 2023, the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) Special Interest Group on Gut Microbiota and Modifications set out updated recommendations for the use of probiotics in the management of selected paediatric gastrointestinal disorders:20
“If the use of probiotics for preventing antibioticassociated diarrhea (AAD) is considered because of the existence of risk factors such as class of antibiotic(s), duration of antibiotic treatment, age, need for hospitalization, comorbidities, or previous episodes of AAD, healthcare professionals may recommend high doses (≥5 billion CFU/day) of S. boulardii or L. rhamnosus GG started simultaneously with antibiotic treatment to prevent AAD in outpatients and hospitalized children (certainty of evidence: moderate; grade of recommendation: strong).”
CLINICAL CASE by Pr. Aldo Maruy
A 10-year-old patient came to the clinic with a seven-day history of diarrhea. From the onset, the child had been producing each day two or three liquid stools with mucus, though without blood. The mother said there had been neither fever nor vomiting. On clinical examination, the child seemed well and appeared to be adequately hydrated.
The doctor requested a stool culture and OVA & parasite checks; these were negative.
An antecedent had not initially been considered: six weeks before, the child had had a respiratory infection which was treated with antibiotics.
Late-onset Antibiotic Associated Diarrhea (AAD) was then suspected. The patient received probiotics and improved within a week.
AAD can take anywhere from 2 hours to 8-10 weeks to develop after antibiotic use.
EXPERT OPINION
Antibiotic Associated Diarrhea (AAD) is a common side effect of antibiotics. Age, spectrum of antibiotics used, underlying illness and recent surgery have been identified as risk factors. Recent evidence shows a new one: composition of the microbiota. In patients treated with β-lactams, higher relative abundances of Bacteroides were inversely associated with AAD while higher baseline abundance of Bifidobacterium species and Lachnospiraceae and amino acid biosynthesis pathways (AABP) were associated with AAD. Relative abundances of potentially protective taxa and levels AABP may distinguish children who did and did not experience AAD. Further studies are needed to investigate whether similar trends are observed across different antibiotic types. The identified potentially protective taxa may inform the development of preventive approaches for AAD.
PR. ALDO MARUY Paediatric Gastroenterologist, Hospital Cayetano Heredia, Lima (Peru)
Pathogenic bacteria such as Shigella, Vibrio cholerae, Salmonella, E. coli… lead to bacterial diarrhea, through mechanisms that depend on the bacteria involved. Bacterial diarrheas are accompanied by intestinal dysbiosis. Symmetrically, the gut microbiota exerts effects on the bacterial infection. Since a ‘healthy’ gut microbiota is more resistant to infection, probiotics could reduce the severity of many bacterial infections.
Underlying how lethal bacterial diarrhea can be, these 8 bacteria were responsible for more than a third of the over 1.65 million deaths from infectious diarrhea recorded worldwide in 2016.2
These 8 bacteria
Shigella: 212,438 deaths.
Vibrio cholerae: 107,290 deaths.
Non-typhoidal Salmonella spp: 84,799 deaths.
Campylobacter spp: 75,135 deaths.
Enterotoxigenic E. coli: 51,186 deaths.
Clostridioides difficile: 22,417 deaths.
Aeromonas: 16,881 deaths.
Enteropathogenic Escherichia coli: 12,337 deaths.
FROM INFECTION TO DIARRHEA
The mechanisms that lead to bacterial diarrhea depend on the bacteria involved. Transmitted via contaminated food, water or by personto-person contact, Shigella infests the gastrointestinal tract, produces an enterotoxin and serotype toxin 1, destroying the intestinal epithelium and leading to severe bloody and mucous diarrhea.3,5
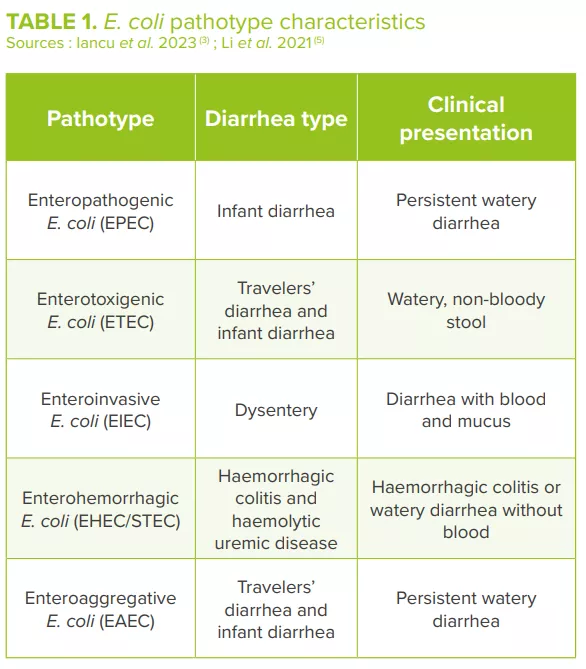
Pathogenic variants of Vibrio cholerae produce a cholera toxin that activates anion secretion, inhibits absorption of electroneutral NaCl and destroys the intestinal barrier function, thereby inducing massive fluid secretion in the lumen of the small intestine and the loss of large amounts of water, sodium, chloride, bicarbonate and potassium.3,5,13 Different pathogenic E. coli strains, classified into different pathotypes (Table 1), cause mild to severe diarrhea usually accompanied by fever. E. coli adheres to the intestinal epithelial cells through the adherent fimbriae, produces toxins and exerts its pathogenic effects.3,5
Image
EFFECT OF PATHOGENS AND DIARRHEA ON MICROBIOTA
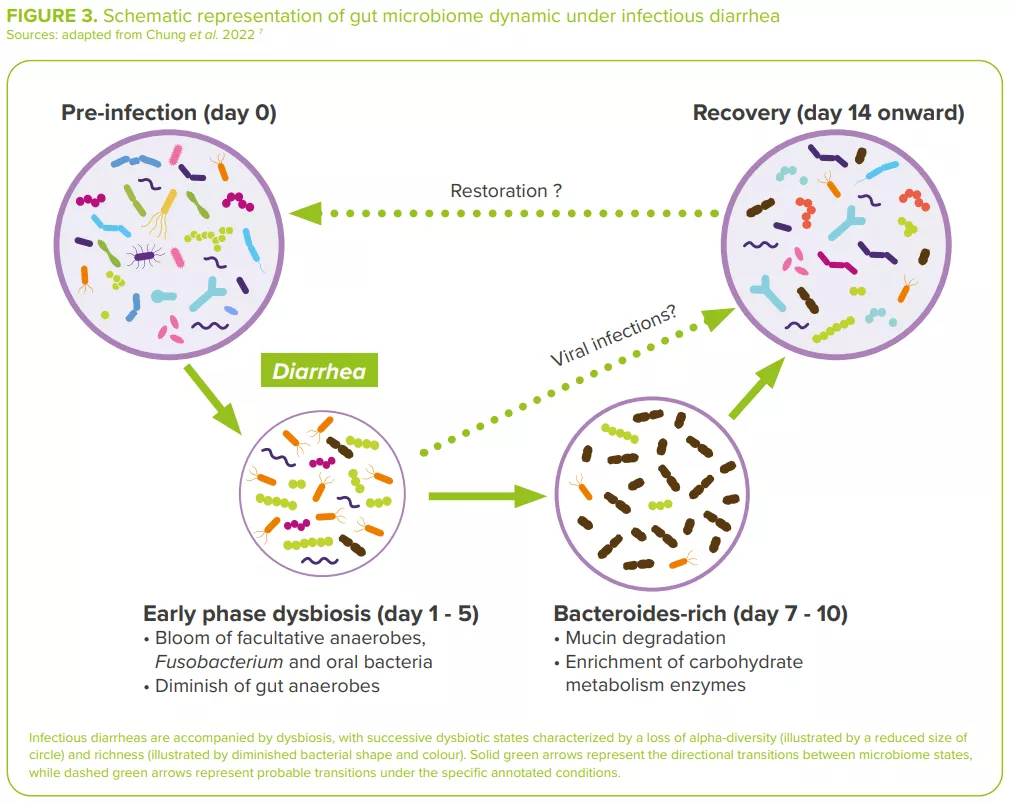
Bacterial diarrheas are accompanied by dysbiosis, usually with an overabundance of facultative anaerobes (Escherichia, Streptococcus, Enterococcus, etc.) in dysenteric diarrhea, and a depletion in bacteria of known immuno-modulatory effects (Lactobacillus ruminis, Bifidobacterium pseudocatenulatum)7 (Figure 3).
Image
For example, in cholera, the gut microbiota is substantially modified both during and after infection, this as a consequence of the removal of the mucus layer along with the residing gut microbial community and of the delivery of toxin byV. cholerae. 13 During recovery, the gut microbiota of cholera patients slowly repopulates via an accumulation pattern similar to that of the maturation of the gut microbiota observed in children.3
In the same way, children infected with diarrheagenic E. coli (DEC) display a distinctive gut microbial composition, with a high fraction of Bacteroidetes and Proteobacteria and a reduced abundance of Firmicutes. 13 Increases in Proteobacteria could be partially explained by an increase in Escherichia/ Shigella species (as the cause of diarrhea) and in other members of Enterobacteriaceae, such as Citrobacter and Enterobacter (related to histamine production induced by proinflammatory environments and associated with E. coli adherence).14 Frequent antimicrobial use can also partly explain the observed dysbiosis.7
GUT MICROBIOTA PROTECTION AGAINST INFECTIONS
Symmetrically, the gut microbiota has demonstrated effects on bacterial infection. In germ-free animals, their lack of a gut microbiota and the absence of ecological competition results in an immature immune system that renders them highly susceptible to diarrheal pathogens: 10 colony-forming units (CFU) of Salmonella are enough to cause a lethal infection, whereas to kill 50% of mice with an intact gut microbiota 103 –109 CFU are required.8
In humans, Prevotella, Bifidobacterium and Blautia have been shown to reduce colonization of V. cholerae. Conversely, Paracoccus is believed to support the growth of the pathogen.13 This is the reason why promoting a ‘healthy’ gut microbiome has been considered a useful approach in the intervention and prevention of cholera.13
“The GI tract encompasses ~1 to 10 times more bacterial cells than the number of cells in the human body.” 16
BACTERIAL AND YEAST PROBIOTICS, PREBIOTICS AND FMT
The severity of several bacterial infections could be reduced by probiotics: for example, probiotic E. coli inhibits the biofilm formation of other E. coli strains and likewise those of the pathogenic Staphylococcus aureus and S. epidermidis. 3 Regarding dysentery, a combination of Lactobacillus and Bifidobacterium strains and a Streptococcus strain reduces both the duration of blood-affected diarrhea and the time spent in hospital.3
Numerous mechanisms could explain why probiotics alleviate diarrhea:3 production of antimicrobial substances, competitive exclusion, competition with cell binding sites, production of acids and metabolites that lower the surrounding pH, strengthening of the gut mucosal barrier, modulation of gut mucosal immunity and gut microbiota diversity. For example, the probiotic yeast Saccharomyces boulardii may facilitate gut microbiota restoration in children with acute diarrhea.15
Prebiotics can also have a positive impact on diarrhea: by increasing the bacterial production of short-chain fatty acids (SCFAs) such as butyrate, which contribute to the gut barrier integrity; and by antagonizing the adherence of pathogens to epithelial cells, thus inhibiting colonization and promoting gut pathogen elimination.3
Fecal microbiota transplantation (FMT), which aims to restore a healthy gut microbiota, has proven effective and is only indicated in the treatment of recurrent C. difficile in both adults and children.14
CLINICAL CASE by Pr. Aldo Maruy
A 2-year-old boy presented with fever, abdominal pain and diarrhea with mucus and blood. He had history of two similar episodes in the last six months, treated solely with antibiotics.
In order to prevent a relapse, it was decided to treat him with antibiotics and probiotics. The diarrhea ceased within 48 hours, the antibiotic was suspended at the 5th day while the probiotic was continued for two weeks; a diet rich in complementary food and prebiotics was prescribed.
In addition to treating the infection with antibiotics, it is recommended in order to prevent a new diarrheal episode that the composition of the gut microbiota be restored via the diet together with the administration of prebiotics and probiotics
EXPERT OPINION
Throughout one’s life, a healthy microbiota plays an important role in the prevention and treatment of bacterial diarrhea. Specific species have demonstrated protective effects against diarrhea: Lactobacillus taxa are protective against Shigella spp.-induced diarrhea; the presence of Sutterella sp., Prevotella copri and Bacteroides vulgatus predict resistance to enterotoxigenic E. coli (ETEC). On the other hand, microbial intervention, through modifying the diet and using prebiotics, probiotics and FMT, can regulate the composition of gut microbiota to prevent and treat diarrhea. Future research should expand our knowledge of the microbiome as it relates to infectious diarrhea, thereby assisting in the design of improved preventative and managerial interventions.
PR. ALDO MARUY Paediatric Gastroenterologist, Hospital Cayetano Heredia, Lima (Peru)
CONSEQUENCES OF TRAVELERS’ DIARRHEA
When visiting medium- and high-risk destinations, 10–70% of travelers from low infectious disease-risk countries experience diarrhea. Travelers’ diarrhea is predominately caused by bacteria (≥80%–90% of cases), with intestinal viruses accounting for a minimum of 5%–15% of the cases.52 Infections by protozoal pathogens might account for approximately 10% of diagnoses mostly in those traveling for extended periods.
The microbiota of travelers who experienced diarrhea show greater variation throughout the length of their stay than those of healthy travelers, associated with a lower baseline diversity, which has been linked to an increased susceptibility to infection.51
Moreover, diarrhea reduces the capacity of microbiota restoration (large increase of the rate of divergence from baseline) and leads to the acquisition of multidrugresistant organisms.51 Thus, according to a study including 267 Americans travelling outside the United States, a third returned with diarrhea, 61% with intestinal dysbiosis and 38% with antibiotic-resistant bacteria (most of them an E. coli), contributing to the global spread of antimicrobial resistance.58
Enriched in diarrhea:
E. coli, Dorea fomigenerans, Bacteroïdes vulgarus, B. caocae, Odoribacter splanchnicus…,
INFECTIOUS DIARRHEA, ONE OF THE LEADING CAUSES OF INFANT MORTALITY WORLDWIDE
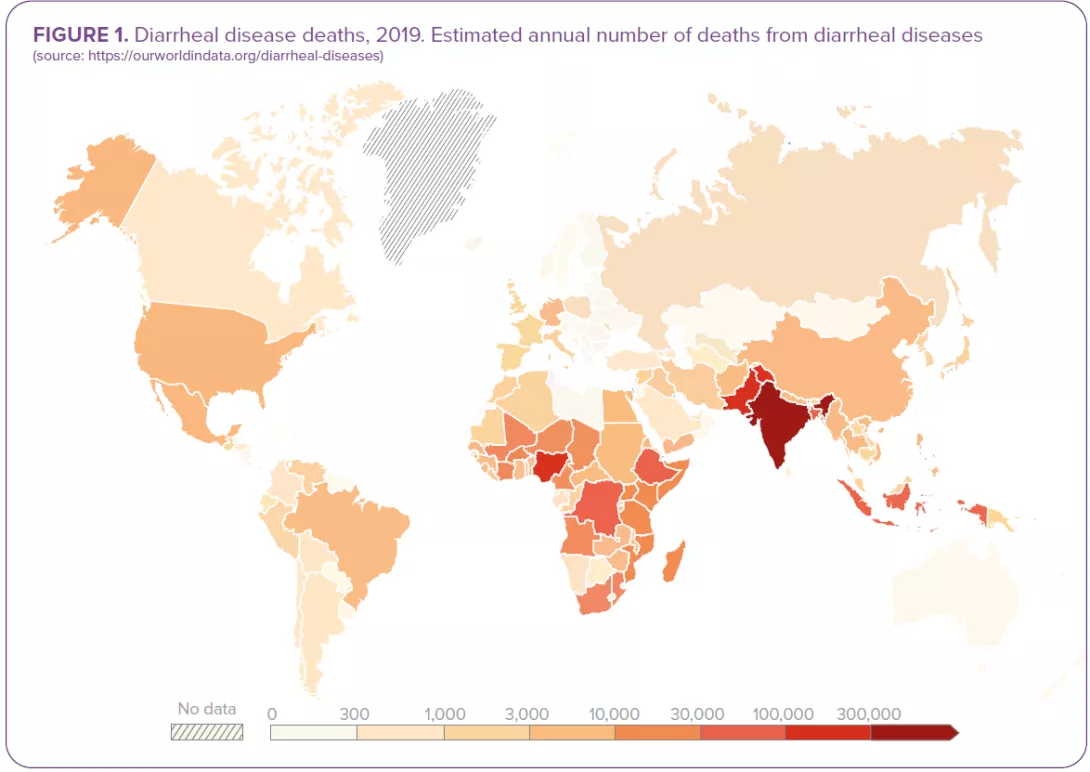
The passage of 3 or more loose or liquid stools per day corresponds to the common definition of diarrhea as set out by the WHO.1 Both criteria (frequency and consistency) are necessary: frequent passing of formed stools is not diarrhea, nor is the passing of loose stools by breastfed babies (Figure 1). 1.6 million deaths were attributed to diarrhea in 2016.2 Children are particularly at risk: diarrheal disease is the 3rd leading cause of death in children under 5 years of age. A large part of the mortality used to be attributed to severe dehydration linked to fluid loss but today, septic bacterial infections account for an increasing proportion of all diarrhea-associated deaths.1 Malnourished or immunity-impaired children are the most at risk of life-threatening diarrhea, as well as people living with HIV.1
DIARRHEA CLASSIFICATION
There are 3 clinical types of diarrhea based on its symptoms and duration:1
acute watery diarrhea, which lasts several hours or days (up to 14 days) and includes cholera;
acute bloody diarrhea (dysentery);
persistent diarrhea, which lasts 14 days or longer.
Most cases of acute diarrhea are due to infections:1,3,4 a virus, bacteria or parasites could all be responsible, but rotavirus and Escherichia coli are the two most common etiological agents of moderate-to-severe diarrhea in low-income countries.1Rotavirus and Shigella are responsible for the highest number of infectious-diarrhea related deaths;2 this is giving rise to preventive vaccination strategies (still under development for the latter). Although certain fungal communities have been confirmed to be associated with diarrhea, the role of fungi in diarrhea remains controversial.5 They could be at work in some clinical settings, especially in immunocompromised patients prone to invasive fungal infections (candidiasis).6
PATHOPHYSIOLOGICAL SYNDROMES OF DIARRHEA
From the clinical perspective, diarrheagenic pathogens can cause 2 pathophysiological syndromes:4
Noninflammatory diarrhea (NID): patients present with nausea, vomiting, watery and voluminous stools, and abdominal cramping resulting from intestinal secretion (the intestinal mucosa remains intact). This milder course of disease is usually viral (Rotavirus, Norovirus…) but it can also be bacterial (enterotoxigenic Escherichia coli, Clostridium perfringens…) or parasitic (Giardia, …);
Inflammatory diarrhea (ID): patients present with fever, abdominal pain, tenesmus and bloody stools of smaller volume than in NID. This severe course of disease is usually caused by invasive or toxinproducing bacterial strains (Shigella, Salmonella species…) that lead to mucosal barrier disruption and tissue destruction.
“Rotavirus and Escherichia coli are the two most common etiological agents of moderate-to-severe diarrhea in low-income countries.”
Image
BEHIND THE SCENES OF DIARRHEA: THE MICROBIOTA
VICIOUS CIRCLE: WHEN DIARRHEA LEADS TO GUT DYSBIOSIS
Infectious diarrhea is regarded as a major dysbiotic event resulting from:
increased bowel movements and disruption to mucosal integrity, 3
increased proportion of water in the fecal matter and reduced transit time which contributes to taxonomic scarcity, 3
and possible oral rehydration, zinc supplements, probiotics and even antimicrobials (in the case of dysentery or bacterial infections) which also contribute to an imbalance in the intestinal microbiota.7
Depending of the type of infection, infectious diarrheas are usually accompanied by dysbiotic states: 7 bacteria-induced diarrhea is generally linked to an elevation in Escherichia, Streptococcus and oral bacteria; viral infections lead to a less pronounced reduction in anaerobic commensals in the gut (higher abundance in Bifidobacterium); giardia-induced diarrhea is linked to a decrease in Gammaproteobacteria and an enrichment in Prevotella.
“The community of microbes that inhabit the gut is as numerous as human cells, with the vast majority of bacteria residing in the colon.” 8
“DYSBIOSIS”
Dysbiosis corresponds to the disruption of a formerly stable, functionally complete microbiota.9
“INTESTINAL MICROBIOTA”
The community of microorganisms - bacteria, viruses, fungi (including yeasts) and parasites - that inhabit the gut.10
VIRTUOUS CIRCLE: WHEN THE GUT MICROBIOTA OFFERS PROTECTION
Mechanisms by which the gut microbiota provides colonization resistance can be both direct and indirect. The microbiota directly inhibits diarrheal pathogens mainly via competition for nutrients, but also by limiting in a variety of ways the growth of diarrheal pathogens: secreting bacteriocins (antimicrobial peptides), cell contact-dependent inhibitory structures (type VI secretion system), producing molecules that reduce the pathogens’ virulence…
The microbiota also indirectly inhibits diarrheal pathogens via its effects on the host: by promoting gut barrier maintenance and by stimulating both the innate and the adaptive immune system.8
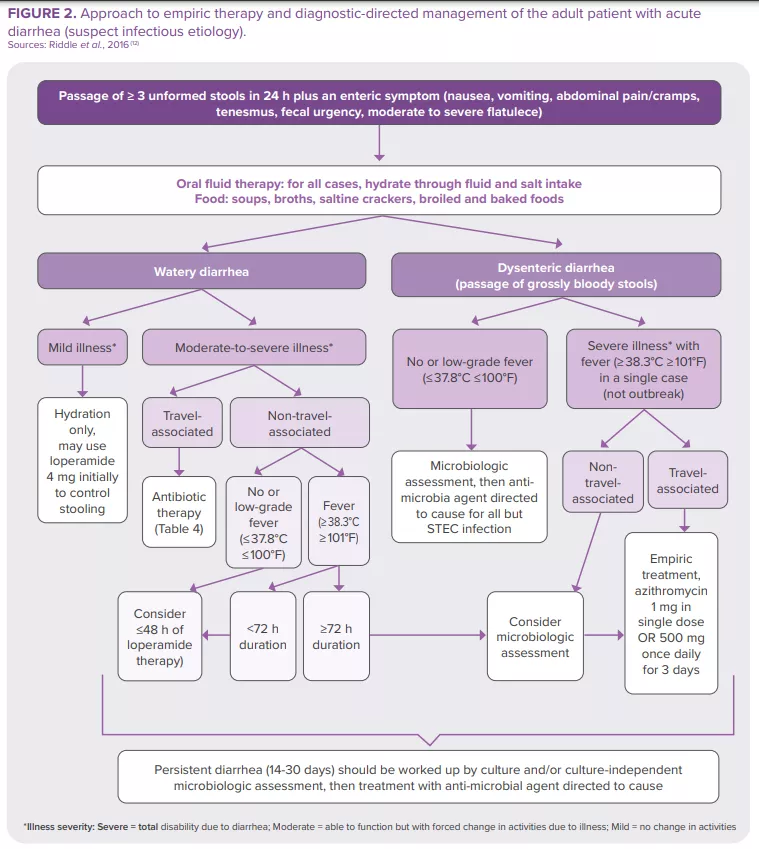
HOW TO MANAGE INFECTIOUS DIARRHEA?
The majority of intestinal infections are self-limiting in immunocompetent individuals. Nevertheless, some patients (with severe dehydration, more severe illness, persistent fever, bloody stools, immunosuppression…) require specific diagnostic investigation. These can include a complete blood count, a creatinine and electrolytes assessment, verification of leukocytes and lactoferrin presence in the stools, stool culture, along with C. difficile testing, PCR, ova and parasites search, endoscopy and abdominal imaging11. The American College of Gastroenterology (ACG) guideline12 provides recommendations for the diagnosis and management of adult patients presenting with acute diarrhea of suspect infectious etiology (Figure 2). Clinical investigation in children is based on the same principles.23 In 2023, World Gastroenterology Organisation Global Guidelines included probiotics in the prevention and treatment of some infectious diarrhea57.
Image
World Gastroenterology Organisation Global Guidelines, 2023
Treatment of acute diarrhea:“oral administration [of some probiotic strains] shortens the duration of acute diarrheal illness in children by approximately 1 day.”57
Prevention of:
acute diarrhea: “probiotics probably make little or no difference with diarrhea lasting 48 hours or longer.”
antibiotic-associated diarrhea: “probiotics may provide a moderate effect for preventing antibiotic-associated diarrhea in children, adults, and elderly adults.”
Clostridioides difficile diarrhea: “probiotics are effective for preventing C. difficile–associated diarrhea in patients receiving antibiotics.”





 Antibiotics: what impact on the microbiota and on our health?
Antibiotics: what impact on the microbiota and on our health?
 6 essential things you should know about antibiotics
6 essential things you should know about antibiotics