According to two studies published in Cell Host & Microbe, a reduction in gut levels of the bacterium F. prausnitzii serves as a biomarker for chronic fatigue syndrome.
Chronic fatigue syndrome, also known as myalgic encephalomyelitis (ME/CFS), is characterized by symptoms such as exhaustion, post-exertional malaise, memory problems, pain, gastrointestinal disturbances, immune abnormalities, and sleep disorders. Even though it affects between 0.4% and 2.5% of the world’s population, mainly adult women aged between 20 and 40 years, this debilitating chronic disease remains poorly understood. However, scientists are studying the role of gut-brain communications 1 in the disease and in particular the involvement of the gut microbiota. By focusing on changes in the microbiota, two recent studies published in the journal Cell Host & Microbe2,3 have sought to better understand the disease and identify potential biomarkers.
Between 0.4% and 2.5%
The global prevalence of ME/CFS ranges between 0.4% and 2.5%.
20 to 40 years of age
The illness predominantly begins in adults 20–40 years of age.
The potential role of butyrate-producing bacteria
In the first study, metagenomic and metabolomic analyses were performed on fecal samples collected from 106 patients and 91 healthy controls living in 5 US states. The study highlights a major gut dysbiosis in CFS patients, with differences between the two groups in terms of gut microbiome diversity, abundance, functional biological pathways, and interactions. Specifically, Faecalibacterium prausnitzii and Eubacterium rectale, two beneficial butyrate-producing bacteria, were depleted in those suffering from chronic fatigue. Further analyses confirmed a lower synthesis of bacterial butyrate in the CFS patients. Moreover, the more F. prausnitzii was depleted, the more severe the fatigue.
Short-term patients vs. long-term patients
The second study, also US-based, included 149 patients and 79 healthy controls, and further distinguished two groups among the patients: 75 patients who had been ill for less than 4 years and 74 patients who had been ill for more than 10 years. Here again, the researchers found a major gut dysbiosis, especially in the short-term patients, with depleted levels of F. prausnitzii. The gut microbiota composition of the long-term patients was closer to that of the healthy controls (with some notable differences in terms of low abundance species and heterogeneity), suggesting a return to relative homeostasis.
On the other hand, these long-term patients presented more severe clinical symptoms and a more greatly altered metabolism than the other patients, including at immune system level. The researchers thus suggest that chronic fatigue may begin with a loss of beneficial bacteria, particularly those that produce butyrate, which then leads to metabolic changes in the host. In some individuals, these modifications may lead to irreversible metabolic and phenotypic changes and thus to an altered state of health over the long term.
However, further research is needed to eliminate potential biases in the analysis, and thus to confirm the researchers’ hypothesis and pave the way for new diagnostic tools and, with any luck, new treatments.
Could a depleted gut bacterium unable to produce enough of a molecule beneficial to our health be behind chronic fatigue syndrome (CFS), also known as myalgic encephalomyelitis (ME)? A team of researchers has taken a closer look. 1
One of the collateral effects of Covid – or more precisely of long Covid – has been to bring an illness presenting similar symptoms, chronic fatigue syndrome (also known as myalgic encephalomyelitis), back under the spotlight.
Definition
Chronic fatigue syndrome, also known as myalgic encephalomyelitis, is a chronic and disabling illness that remains unexplained. The illness is characterized by a range of symptoms, including fatigue, post-exertional malaise, memory problems, pain, gastrointestinal disturbances, immune abnormalities, and sleep disturbances.
This chronic disease mainly affects women aged between 20 and 40, and its symptoms include debilitating fatigue, post-exertional malaise, memory problems, gastrointestinal disturbances, immune abnormalities, and sleep disorders. Two studies published in the journal Cell Host & Microbe explore this mysterious disease, and more particularly its links to the gut microbiota.
Between the ages of 20 and 40
The illness predominantly begins in adults 20–40 years of age.
Depleted microbiota observed in chronic fatigue syndrome
Both studies showed depleted levels of a gut bacterium called Faecalibacterium prausnitzii in CFS patients. Moreover, the more F. prausnitzii was depleted, the more severe the fatigue. But that’s not all. This bacterium is known to produce a (sidenote:
Short chain fatty acids (SCFA)
Short chain fatty acids (SCFA) are a source of energy (fuel) for an individual’s cells. They interact with the immune system and are involved in communication between the intestine and the brain.
Silva YP, Bernardi A, Frozza RL. The Role of Short-Chain Fatty Acids From Gut Microbiota in Gut-Brain Communication. Front Endocrinol (Lausanne). 2020;11:25.) called butyrate, which is beneficial to our health. Butyrate protects our gut barrier and modulates the immune system, and far from staying confined in the digestive system, it also enters the bloodstream, where it provides further benefits.
Between 0.4% and 2.5% of the world’s population
The global prevalence of ME/CFS ranges between 0.4% and 2.5%.
Disrupted immune system
The second study appears to show that this SCFA may determine the long-term clinical course of the disease. In patients who have suffered from CFS for more than ten years, the gut microbiota seems to return to balance over time (although some differences persist compared to healthy people). But long-term patients had more severe symptoms and their immune system seemed more disturbed than that of patients who had suffered from the disease for less than four years. According to the researchers, initial disturbances of the gut microbiota and a decrease in butyrate may, in some people, lead to irreversible changes across the whole body, which in turn lead to an altered state of health over the long term. 2
3 females vs. 1 male in average
The illness is more common in females than males with a ratio averaging about 3/1, ranging as high as 6/1.
You are a researcher with an innovative and evidence-based research showing a clear link between gut microbiota and diseases or a link between digestive disorders and microbiota? With a concrete clinical application? You have already published your work and want to share it with an international audience?
What about being published in an international journal in 5 languages available in paper and digital version!
Microbiota Mag, the expert microbiota magazine, offers you the opportunity to publish an original sum-up of your article on gut microbiota & health & diseases.
Dare to apply!
Please ensure you consult the "Article file" and "Criteria" sections below before applying
Article file
2,500 words (spaces included). This short article must be written in English. It must:
be sent via the form below
contain competing interests (no conflict of interest…), data availability statement… Please provide sufficient detail to avoid delays in processing your paper;
include references list formatted in line with Microbiota Mag’s editorial charter:
3 autors, et al. Titre. Paper’s name (italics). Year of publication, volume, edition, number of pages + insert the PubMed hypertext link.
Criteria
The call for papers is open to all physicians, PhD's and Pharm-D's working in gastroenterology, pediatrics, microbiology, infectious diseases, internal medicine….
We will consider only research in gut microbiota field
The objective is to support researchers; we will consider researchers that recently started to publish in scientific peer reviewed journals (from 2015 until now)
Papers under submission will not be considered (or published on bioRxiv.org)
There are no geographic limitations of applicants.
All applications will be reviewed by an independent scientific committee according to the following criteria:
In April 2023, to mark IBS Awareness Month, the Biocodex Microbiota Institute has launched “Patient Stories”, a series of video testimonials from patients suffering from IBS. In this dedicated page, discover the testimonies of patients suffering from different pathologies somehow linked to their microbiota.
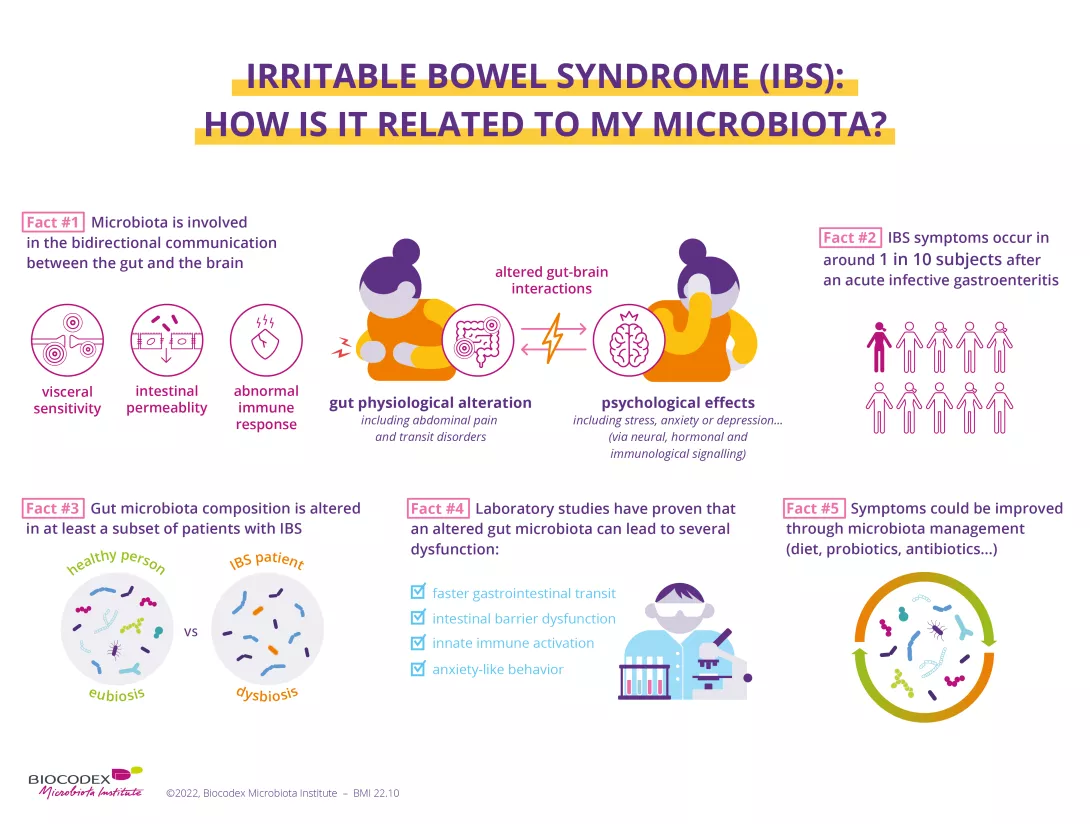
Irritable bowel syndrome (IBS), previously called a “functional bowel disorder”, is the most common gut-brain axis disorder. Symptoms include recurrent abdominal pain, bloating and bowel dysfunction. Its main symptoms involve the bowels, but IBS can often also be associated with anxiety and depression. We have now established links with communication disruptions in the gut-brain axis, in which gut microbiota play a role.
Disorders of Gut-Brain Interaction (DGBI) are also known as “functional bowel disorders”. We say they are “functional” because there are no structural abnormalities of the digestive organs or tissues. Other terms used for irritable bowel syndrome (IBS) include “functional colopathy”, “spastic colitis” and “irritable colon syndrome” 2.
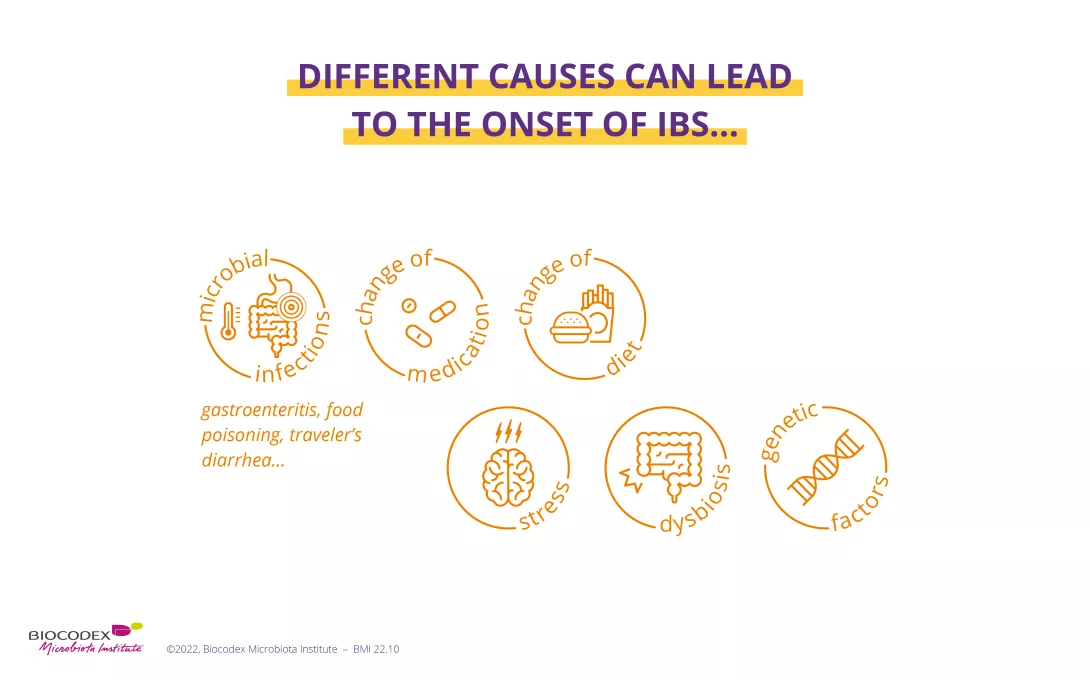
What causes irritable bowel syndrome?
The causes of irritable bowel syndrome are complex, and not yet fully identified. IBS is thought to be triggered by a combination of different factors, the importance of which varies from person to person 2: genetic predisposition, certain medical histories and treatments, stress, diet, etc.
The most well-known risk factor for IBS is a history of acute intestinal infection: 10% of people with IBS believe their problems began after such an episode, for example viral gastroenteritis, traveler’s diarrhea or (sidenote:
Diverticulitis
Diverticulitis is an inflammation or infection of the diverticula, small folds (hernias) in the inner wall of the colon.
https://www.cancer.gov/publications/dictionaries/cancer-terms/def/diverticulitis) 1,4,5. The risk of developing IBS seems to be quadrupled after one year following this type of infection 1.
2 out of 3
IBS sufferers in Western countries are women.
50
The frequency of IBS decreases after the age of 50.
Recent research is increasingly suggesting that the gut microbiota play a key role in the development of IBS 6,7. Experts have even recognized an imbalance in the composition of the gut microbiota, or dysbiosis, as a plausible cause of IBS 5. Antibiotic-induced dysbiosis has also been associated with the development of IBS 1.
The scientific community is also showing strong interest in the role of diet in IBS. Over 60% of IBS patients say their symptoms appeared or worsened after eating 8,9. This is labeled as bowel hypersensitivity. The presence of certain food compounds (wheat, milk, etc.) appears to trigger an exaggerated reaction in the gut, which can be immune-related 10,11. Moreover, dietary habits often disturb the gut microbiota and cause abnormal fermentation of ingested food, thought to play a crucial role in intestinal distension 10.
IBS is also triggered by traumatic or distressing events (bereavement, divorce, abuse, conflict, etc.), and by acute or chronic stress and other psychological disorders such as depression or anxiety 1,2,7. These appear to exert a negative impact on the (sidenote:
The enteric nervous system
The enteric nervous system (ENS) is the nervous system of the gut. It is composed of a network of neurons that line the walls of the gastrointestinal tract and controls the sensory, motor and secretory activity of the digestive system.
Watson C., Kirkcaldie M., Paxinos G. The brain: an introduction to functional neuroanatomy – Chapter 4 - Peripheral nerves. Academic Press, 2010. 43-54), which controls motor function, the mucosal barrier, sensory function and intestinal secretions 1.
Could poor communication between the gut and brain explain IBS?
Does the gut-brain axis mean anything to you? The brain communicates with the enteric nervous system in both directions: what happens in the brain affects the gut, and vice versa. But that is not all: neurons in the gut are linked directly to the gut microbiota, which also maintains bidirectional communication with our hormonal and immune systems.
gut hypersensitivity and impairment of pain control in the central nervous system
the brain perceives normal gut movements as pain;
intestinal motility disorders
the intestines contract abnormally;
disturbances of the intestinal immune system
(in 50% of cases), excessive immune stimulation after an infection 5 or hypersensitivity to certain foods 6;
impaired intestinal barrier integrity
fragments of bacteria are able to pass out of the gut, causing chronic diffuse inflammation 7,12;
gut dysbiosis
occurs in 2 out of 3 of people with IBS, and is potentially involved in all the above IBS disturbances and symptoms 2,7.
What are the main symptoms of IBS?
According to well-established criteria, IBS is characterized by the simultaneous presence of several symptoms, involving abdominal pain and bowel dysfunction. These symptoms must be sufficiently frequent and long-standing (>1 day/week in the past 3 months) 13,14:
Recurrent abdominal pain (at least 1 day a week);
Painful defecation;
Bloating;
Change in stool consistency;
Change in stool frequency.
Some clarification and explanation may be useful!
Abdominal pain is manifested by spasms, burning sensations, tightness and bloating. It occurs around the navel, in the lower abdomen, and can appear to follow the course of the colon. The pain is associated with defecation, and can be aggravated or relieved by the emission of gas or stools 2.
Abnormalities in stool consistency and frequency range from stools that are too soft and/or too frequent (as in diarrhea) to stools that are too hard and/or too infrequent (as in constipation). There may be alternating periods of diarrhea and constipation. These transit disorders are sometimes accompanied by other types of discomfort, including an urgent need to pass stools, presence of mucus in stools or an impression of incomplete stool evacuation 5.
These changes in stool frequency and consistency allow IBS to be classified as one of four subtypes:
IBS-C: Constipation predominant IBS (at least 1 in 4 stools);
IBS-D: Diarrhea predominant IBS (at least 1 in 4 stools);
IBS-M: Mixed diarrhea and constipation IBS (at least 1 in 4 stools are constipation predominant, and 1 in 4 are diarrhea predominant). This is the most common subtype (40% of people with IBS);
IBS-U: Unclassified IBS, not meeting the criteria for IBS-C, D or M. Abnormal stools are rare 15,16.
It is worth noting that someone with IBS can develop a different subtype over time 3.
IBS symptoms vary in severity from person to person, and over time in the same person 3,5. They can range from being inconvenient to very disabling, with severe forms of IBS affecting 20-25% of patients 3. Generally speaking, they affect personal, social and professional quality of life 1,3.
Only physicians can diagnose IBS, once they have successfully ruled out another digestive disorder 2. There is no diagnostic test for IBS as yet, so physicians rely on patients’ descriptions of symptoms; the results of clinical examinations and imaging carried out in people with IBS are generally normal 3.
Which disorders and conditions are associated with IBS?
Generally speaking, people with IBS are more likely to suffer from certain disorders and conditions.
Other digestive disorders: In over 20% of cases, IBS is accompanied by bloating, flatulence 4, nausea or heartburn 16. Some people are also intolerant of certain foods 5.
Psychological disorders: Not only can psychological factors play a role in causing IBS, but a proportion of sufferers may also develop psychological disorders as a result of IBS 1, for example anxiety, stress, depression, insomnia or eating disorders 5.
Genitourinary disorders: IBS may be accompanied by pelvic pain, urinary disorders, pain during intercourse in women and erectile dysfunction in men 4,5.
Endometriosis: Studies have shown that women with endometriosis are three times more likely to develop IBS 17.
General disorders: Some people with IBS experience fatigue, lethargy, headaches and/or muscle pain 2,4,5. IBS is more common in people with fibromyalgia and chronic fatigue 1.
Although painful and challenging to live with in everyday life, IBS is a benign disorder 2. Despite this, IBS symptoms should be relieved as soon as possible to improve quality of life 3. Your physician will give you lifestyle tips and recommend an optimal combination of specific medications and alternative solutions.
Good nutritional habits can alleviate IBS symptoms 6,18:
eat meals at regular times and avoid skipping meals;
avoid “pantagruelian” meals and spicy or greasy dishes;
chew food well;
drink enough fluids;
limit alcohol, caffeine and tobacco;
engage in regular physical activity.
Medication
Some IBS symptoms can be improved by taking physician-prescribed medication, for example antispasmodics, intestinal transit regulators, laxatives in case of IBS-C, antidiarrheals in case of IBS-D, and sometimes antidepressants 9. But these drugs are not effective in everyone 16, and to date none have been shown to relieve all IBS symptoms.
Many people with IBS find that certain foods improve or aggravate their symptoms, but they are not the same for everyone. Modifying the diet can therefore improve IBS symptoms, but this should always be done with the help of a health professional (physician, dietician), to work out a personalized solution and prevent any nutritional imbalance 16.
For example, your physician can help you detect any foods that “don’t work for you” (milk, wheat, legumes, etc.), to then limit their intake 9. You can also include more fiber in your diet if you have IBS-C, although not in excess to avoid increased risk of pain and bloating 6.
Of the diets tested scientifically, the low FODMAPS diet (Fermentable Oligosaccharides, Disaccharides, Monosaccharides and Polyols), seems to give the best results in relieving IBS 6,16 although it does not work for everyone 2. FODMAPs are sugars that are poorly absorbed in the small intestine and ferment through the action of gut microbiota bacteria. This fermentation exacerbates bloating and pain in people with IBS.
The diet consists in significantly reducing intake of foods rich in FODMAPs, which are foods containing lactose, certain cereals, certain fruits and vegetables, synthetic sweeteners, processed foods, etc. It can be restrictive, it requires supervision by a physician, and must be monitored for 4 to 6 weeks. If symptoms improve, foods containing FODMAPs are then gradually reintroduced one by one. In this way it will be possible to determine which food(s) aggravate your symptoms and avoid them 2,19.
Probiotics, prebiotics and fecal microbiota transplantation
Various studies have highlighted the importance of the gut microbiota in the occurrence of IBS, and shown differences in the composition of gut microbiota between affected and healthy individuals 5. Solutions may therefore be proposed to modulate the gut microbiota, with the aim of improving IBS symptoms 20.
According to experts, prebiotics are a promising option. Studies show that they have an overall positive effect on IBS symptoms by acting on various mechanisms, such as visceral hypersensitivity and intestinal motility 9. Probiotics can strengthen the colonic barrier, reduce inflammation and improve gut immunity, for example 20. Some may even act on the gut-brain axis and improve depressive symptoms 9. All these effects appear to be beneficial to well-being: in a recent study, consumption of a strain of bifidobacteria reduced symptom severity and improved quality of life in 60% of people with IBS in 30 days 21.
Studies on the effect of symbiotics on IBS, which combine probiotics and prebiotics, are also underway 9, and initial testing of fecal microbiota transplantation has yielded encouraging results in some patients with IBS who have seen an improvement in both symptoms and quality of life 1.
62%
of respondents thought that consuming probiotics helped to maintain healthy microbiota balance and function
The ultimate microbiota dictionary, brimming with practical tools and inforgraphics to elevate your practice and enlighten your patients, to help them in their microbiota journey.
To increase awareness about Irritable Bowel Syndrome (IBS), the Microbiota Institute is handing the floor to an expert in the field, Pr. Premysl Bercik, clinician and researcher at McMaster University, Canada.
What are the symptoms? Why do I develop IBS? Is it linked to the microbiota? Is there a microbiota-gut-brain axis? All your questions answered here.
IBS is a disorder of gut–brain interaction, which is characterized by chronic abdominal pain and altered bowel habit (changes in stool frequency or stool form) in the absence of any tissue damage. Gastrointestinal symptoms do not come alone as IBS is often accompanied by psychological upset (anxiety, stress or depression). 1
"During the last decade, increasing attention has been given to gut microbiota as a key player in IBS."
Pr. Premysl Bercik
How many people suffer from IBS?
Prof. Premysl Bercik: Data differ between countries, but it is estimated that IBS affects around 5 to 10% population globally. 2 Women are almost twice as likely as men to have IBS. They also report more fatigue and psychological distress. For both men and women, IBS can develop at any age, but its onset is often between age of 20 and 30.
5 to 10%
It is estimated that IBS affects around 5 to 10% population globally.
2 out of 3
patients are women.
The quality of life of IBS patients is severely affected, interfering with their everyday life, frequently resulting in missing work or school. 3
P.-B.:IBS is a complex disorder, its genesis is likely multifactorial and not fully understood. In general, it stems from impaired gut–brain interaction, a bidirectional communication between the digestive tract and the central nervous system. There are several peripheral mechanisms involved in IBS, including intestinal hypersensitivity, altered bowel motility, increased intestinal permeability and low-grade inflammation. In the brain, the signals from the bowel may be incorrectly interpreted and further magnified, and then the brain sends erroneous signals to the gut. During the last decade, increasing attention has been given to gut microbiota as a key player in IBS 4,5.
What is the scientific evidence for the involvement of the gut microbiota in IBS?
P.-B.:There are several lines of evidence that implicate microbiota in IBS:
First, bowel infection (gastroenteritis) is the strongest risk factor for IBS, with 11-14% of patients developing chronic symptoms after acute infection with pathogenic bacteria (Salmonella, E. coli or Campylobacter infection). 6
Second, clinical studies showed that microbiota-directed treatments affect IBS symptoms. Indeed, certain antibiotics improve symptoms in some patients with IBS, while in asymptomatic individuals they can trigger IBS symptoms. Specific probiotics were shown to improve symptoms of IBS, such as abdominal pain, diarrhea or bloating, although there is currently no consensus on which probiotics to recommend in clinical practice. 2
Third, gut microbial composition and metabolic activity differ between IBS patients and healthy individuals, and associate not only with bowel symptoms, but also with anxiety and depression. However, the results from individual studies vary and there seems to be no unique microbial profile that could be attributed to IBS. 7
Finally, and most importantly, several studies have shown that gut dysfunction and associated anxiety can be transferred through microbiota transplantation from IBS patients into germ-free mice. 8,9,10
You’ve talked about gut-brain interaction. Is there a microbiota-gut-brain axis?
P.-B.:The gut-brain axis involves immune, neural and hormonal signaling and growing evidence suggests that the gut microbiota plays a key role in this communication. Although most data have been obtained from animal studies, many clinical studies support this concept. 11 Just to mention few, sudden changes in behavior have been described in patients treated with antibiotics. A recent population-based study found that use of antibiotics in early childhood is associated with an increased risk of developing mental health disorders in later life. The most obvious case comes from patients with end-stage liver disease (cirrhosis), diagnosed with (sidenote:
Hepatic encephalopathy (HE)
Hepatic encephalopathy (HE) refers to changes in the brain that occur in patients with advanced, acute (sudden) or chronic (long-term) liver disease. It is one of the major complications of cirrhosis.
https://britishlivertrust.org.uk/information-and-support/living-with-a-liver-condition/liver-conditions/hepatic-encephalopathy/) These patients display altered behavior and cognition which improve quickly and dramatically after administration of antibiotics or laxatives, or fecal microbiota transplantation 12. And multiple studies found that the microbial profiles differ between patients with psychiatric disorders and healthy individuals. 13
5 take home messages for Irritable Bowel Syndrome (IBS):
IBS is characterized by abdominal pain and altered bowel habits.
Its prevalence is around 5 to 10%, predominantly affecting women, it has a significant socio-economic impact.
Its pathophysiology is not fully understood, it is considered to be a disorder of the gut-brain interaction.
Accumulating animal and clinical data suggest that gut bacteria are involved in cognition, behavior and mood disorders (depression, anxiety…).
Several lines of evidence implicate gut microbiota in IBS:
Bacterial gastroenteritis is the most significant risk factor for IBS.
Microbiota-directed treatments (antibiotics, probiotics) can improve IBS symptoms.
Microbiota profiles and metabolism differ in patients with IBS and healthy individuals.
Transfer of microbiota from patients with IBS induces gut dysfunction and altered behavior in germ-free mice.
Can we modulate the gut microbiota to improve mental health?
P.-B.:In animal models, certain probiotics have shown beneficial effects on behavior and brain chemistry, suggesting they could be used therapeutically in mental disorders. The results of the few clinical studies completed so far suggest that probiotics, if used as an adjunctive treatment, improve symptoms in patients with major depressive disorder. 13 And our recent pilot study found that probiotic treatment improved depression scores and bowel symptoms in patients with IBS, and changed their brain activation patterns. 14 Altogether, this suggest that some probiotics could be helpful not only for patients with functional bowel disorders, but also for those with mental health issues. However, this needs to be confirmed by larger rigorous clinical studies.
Image
BMI-23.14
Please note
The Biocodex Microbiota Institute’s goal is to educate the general public and healthcare professionals about the human microbiota. It does not provide medical advice. Please consult a health professional for any questions or requests you may have.
Get in-depth analyses and expert opinions on topics related to microbiota. Aimed at healthcare professionals, this page offers insights from specialists explaining the link between microbiota and health.
Everything you have to know about microbiota. Biocodex Microbiota Institutes provides you thematic pages gathering reliable and updated contents to share with your patients.
Understanding microbiota. Different experts at the core of microbiota research explain the latest scientific breakthrough revealing the central role of microbiota.




 Fibromyalgia: microbial bile acids associated with symptom severity?
Fibromyalgia: microbial bile acids associated with symptom severity?
 The gut microbiota has a specific signature for fibromyalgia
The gut microbiota has a specific signature for fibromyalgia